Department of Sociology, Ghent University, Ghent, Belgium.
BMC Health Serv Res. 2010 Sep 10;10:268. doi: 10.1186/1472-6963-10-268.
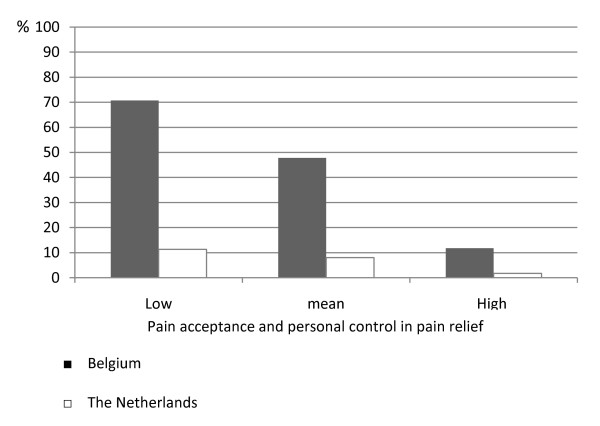
A cross-national comparison of Belgian and Dutch childbearing women allows us to gain insight into the relative importance of pain acceptance and personal control in pain relief in 2 maternity care models. Although Belgium and the Netherlands are neighbouring countries sharing the same language, political system and geography, they are characterised by a different organisation of health care, particularly in maternity care. In Belgium the medical risks of childbirth are emphasised but neutralised by a strong belief in the merits of the medical model. Labour pain is perceived as a needless inconvenience easily resolved by means of pain medication. In the Netherlands the midwifery model of care defines childbirth as a normal physiological process and family event. Labour pain is perceived as an ally in the birth process.
Women were invited to participate in the study by independent midwives and obstetricians during antenatal visits in 2004-2005. Two questionnaires were filled out by 611 women, one at 30 weeks of pregnancy and one within the first 2 weeks after childbirth either at home or in a hospital. However, only women having a hospital birth without obstetric intervention (N = 327) were included in this analysis. A logistic regression analysis has been performed.
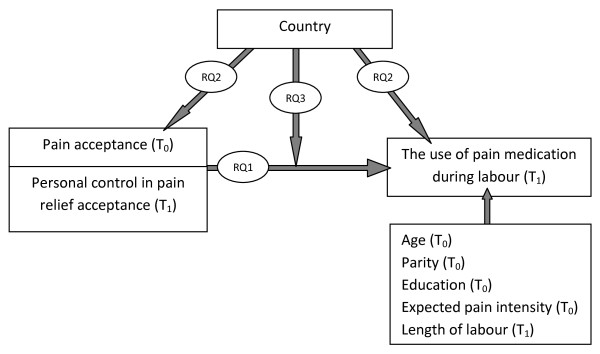
Labour pain acceptance and personal control in pain relief render pain medication use during labour less likely, especially if they occur together. Apart from this general result, we also find large country differences. Dutch women with a normal hospital birth are six times less likely to use pain medication during labour, compared to their Belgian counterparts. This country difference cannot be explained by labour pain acceptance, since - in contrast to our working hypothesis - Dutch and Belgian women giving birth in a hospital setting are characterised by a similar labour pain acceptance. Our findings suggest that personal control in pain relief can partially explain the country differences in coping with labour pain. For Dutch women we find that the use of pain medication is lowest if women experience control over the reception of pain medication and have a positive attitude towards labour pain. In Belgium however, not personal control over the use of pain relief predicts the use of pain medication, but negative attitudes towards labour.
Apart from individual level determinants, such as length of labour or pain acceptance, our findings suggest that the maternity care context is of major importance in the study of the management of labour pain. The pain medication use in Belgian hospital maternity care is high and is very sensitive to negative attitudes towards labour pain. In the Netherlands, on the contrary, pain medication use is already low. This can partially be explained by a low degree of personal control in pain relief, especially when co-occurring with positive pain attitudes.
对来自比利时和荷兰的产妇进行跨国比较,有助于我们深入了解在两种不同的产时照护模式下,疼痛接受度和个人控制对缓解疼痛的相对重要性。尽管比利时和荷兰是邻国,语言、政治制度和地理位置相同,但两国的医疗保健组织存在差异,尤其是在产时照护方面。在比利时,人们强调分娩的医疗风险,但对医疗模式的优点深信不疑,这使风险得到了一定程度的化解。人们认为分娩疼痛是一种不必要的不便,可以通过止痛药轻松解决。在荷兰,助产士模式将分娩定义为一种正常的生理过程和家庭事件。分娩疼痛被视为分娩过程中的盟友。
2004-2005 年,独立的助产士和产科医生在产前检查时邀请妇女参与研究。611 名妇女填写了两份问卷,一份在怀孕 30 周时填写,另一份在分娩后两周内填写,地点在家中或医院。然而,只有接受无产科干预的医院分娩的妇女(N=327)被纳入本分析。进行了逻辑回归分析。
分娩疼痛接受度和缓解疼痛的个人控制使分娩时使用止痛药的可能性降低,尤其是当这两者同时出现时。除了这个一般结果外,我们还发现了很大的国家差异。与比利时产妇相比,在医院正常分娩的荷兰产妇在分娩时使用止痛药的可能性要低 6 倍。这种国家差异不能用分娩疼痛接受度来解释,因为——与我们的工作假设相反——在医院分娩的荷兰和比利时妇女的分娩疼痛接受度相似。我们的研究结果表明,缓解疼痛的个人控制可以部分解释应对分娩疼痛的国家差异。对于荷兰妇女,如果她们能够控制止痛药的使用,并对分娩疼痛持积极态度,那么使用止痛药的可能性最低。然而,在比利时,并不是对缓解疼痛的个人控制预测止痛药的使用,而是对分娩的消极态度。
除了个体水平的决定因素,如分娩时间或疼痛接受度,我们的研究结果表明,产时照护背景对分娩疼痛管理的研究至关重要。比利时医院产科的止痛药使用率很高,而且对分娩疼痛的消极态度非常敏感。相比之下,荷兰的止痛药使用率较低。这在一定程度上可以解释为缓解疼痛的个人控制程度较低,尤其是当与积极的疼痛态度同时出现时。