Norton Leatherman Spine Center, Louisville, KY, USA.
Spine (Phila Pa 1976). 2011 Mar 15;36(6):490-4. doi: 10.1097/BRS.0b013e3181d323f3.
Cross-sectional cohort.
This study aims to provide an algorithm to estimate Short Form-6D (SF-6D) utilities using data from the Neck Disability Index (NDI), neck pain, and arm pain scores.
Although cost-utility analysis is increasingly used to provide information about the relative value of alternative interventions, health state values or utilities are rarely available from clinical trial data. The Neck Disability Index (NDI) and numerical rating scales for neck and arm pain are widely used disease-specific measures in patients with cervical degenerative disorders. The purpose of this study is to provide an algorithm to allow estimation of SF-6D utilities using data from the NDI, and numerical rating scales for neck and arm pain.
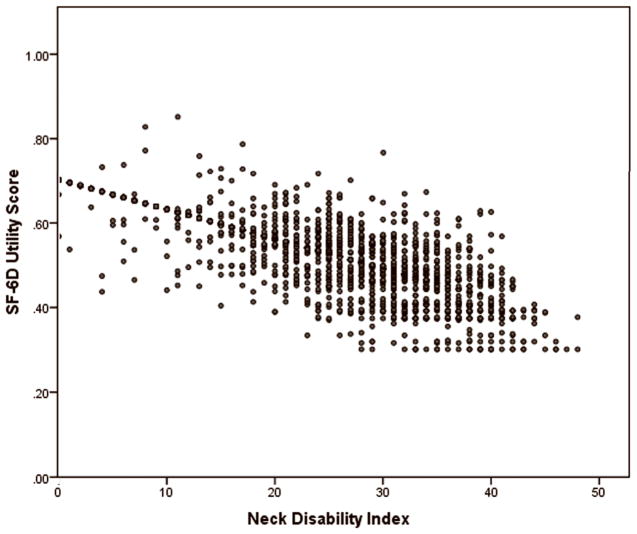
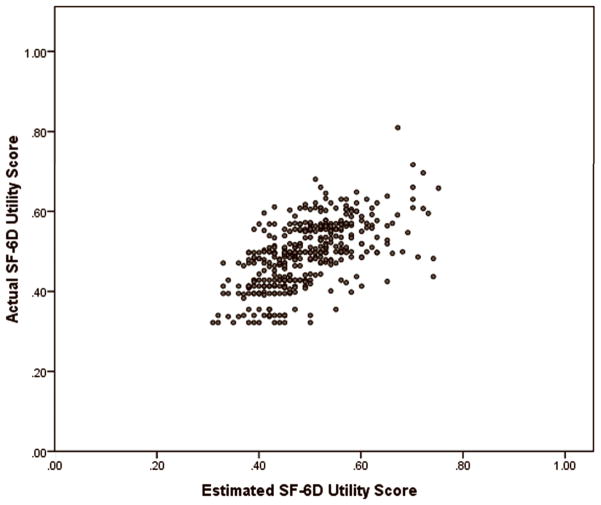
SF-36, NDI, neck and arm pain rating scale scores were prospectively collected before surgery, at 12 and 24 months after surgery in 2080 patients undergoing cervical fusion for degenerative disorders. SF-6D utilities were computed, and Spearman correlation coefficients were calculated for paired observations from multiple time points between NDI, neck and arm pain scores, and SF-6D utility scores. SF-6D scores were estimated from the NDI, neck and arm pain scores were estimated using a linear regression model. Using a separate, independent dataset of 396 patients in which NDI scores were available, SF-6D was estimated for each subject and compared to their actual SF-6D.
The mean age for those in the development sample was 50.4 ± 11.0 years and 33% were male. In the validation sample, the mean age was 53.1 ± 9.9 years and 35% were male. Correlations between the SF-6D and the NDI, neck and arm pain scores were statistically significant (P < 0.0001) with correlation coefficients of 0.82, 0.62, and 0.50, respectively. The regression equation using NDI aloneto predict SF-6D had an R of 0.66 and a root mean square error of 0.056. In the validation analysis, there was no statistically significant difference (P 5 0.961) between actual mean SF-6D (0.49 6 0.08) and the estimated mean SF-6D score (0.49 6 0.08), using the NDI regression model.
This regression-based algorithm may be a useful tool to predict SF-6D scores in studies of cervical degenerative disease that have collected NDI but not utility scores.
横断面队列研究。
本研究旨在提供一种使用颈痛障碍指数(NDI)、颈部和手臂疼痛评分来估算简短六维健康量表(SF-6D)效用值的算法。
尽管成本效用分析越来越多地用于提供有关替代干预措施相对价值的信息,但很少有临床试验数据提供健康状态值或效用值。颈痛障碍指数(NDI)和颈部及手臂疼痛数字评分量表是颈椎退行性疾病患者中广泛使用的疾病特异性测量工具。本研究的目的是提供一种算法,以便使用 NDI 以及颈部和手臂疼痛的数字评分量表来估算 SF-6D 效用值。
2080 例颈椎融合术治疗退行性疾病的患者,前瞻性地收集了术前、术后 12 个月和 24 个月的 SF-36、NDI、颈部和手臂疼痛评分量表评分。计算了 SF-6D 效用值,并计算了 NDI、颈部和手臂疼痛评分与 SF-6D 效用评分之间多个时间点配对观察的斯皮尔曼相关系数。使用线性回归模型从 NDI 估算 SF-6D 评分,从颈部和手臂疼痛评分估算 SF-6D 评分。使用另一组 396 例可获得 NDI 评分的患者的独立数据集,对每位患者进行了 SF-6D 估算,并将其与实际的 SF-6D 进行了比较。
发展样本的平均年龄为 50.4 ± 11.0 岁,33%为男性。验证样本的平均年龄为 53.1 ± 9.9 岁,35%为男性。SF-6D 与 NDI、颈部和手臂疼痛评分之间的相关性具有统计学意义(P < 0.0001),相关系数分别为 0.82、0.62 和 0.50。仅使用 NDI 进行预测的回归方程的 R 为 0.66,均方根误差为 0.056。在验证分析中,实际平均 SF-6D(0.49 ± 0.08)与使用 NDI 回归模型估计的平均 SF-6D 评分(0.49 ± 0.08)之间无统计学差异(P 5 0.961)。
该基于回归的算法可能是一种有用的工具,可用于在收集了 NDI 但未收集效用评分的颈椎退行性疾病研究中预测 SF-6D 评分。