MRC/CSO Social and Public Health Sciences Unit, Glasgow, UK.
Int J Obes (Lond). 2011 Jun;35(6):838-51. doi: 10.1038/ijo.2010.207. Epub 2010 Oct 5.
To investigate the relationship between body mass index (BMI), waist circumference (WC) or waist-hip ratio (WHR) and all-cause mortality or cause-specific mortality.
Cross-sectional surveys linked to hospital admissions and death records.
In total, 20,117 adults (aged 18-86 years) from a nationally representative sample of the Scottish population.
Cox proportional hazards models were used to estimate hazard ratios (HRs) for all-cause, or cause-specific, mortality. The three anthropometric measurements BMI, WC and WHR were the main variables of interest. The following were adjustment variables: age, gender, smoking status, alcohol consumption, survey year, social class and area of deprivation.
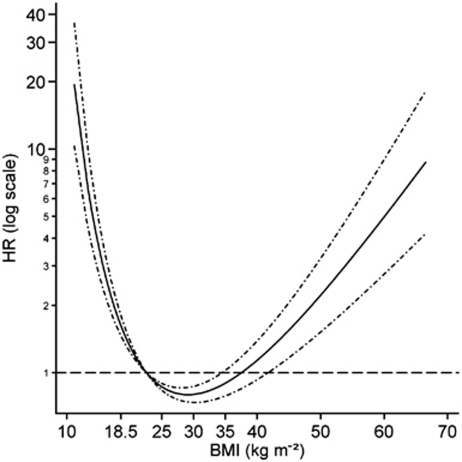
BMI-defined obesity (≥ 30 kg m(-2)) was not associated with increased risk of mortality (HR = 0.93; 95% confidence interval = 0.80-1.08), whereas the overweight category (25-<30 kg m(-2)) was associated with a decreased risk (0.80; 0.70-0.91). In contrast, the HR for a high WC (men ≥ 102 cm, women ≥ 88 cm) was 1.17 (1.02-1.34) and a high WHR (men ≥ 1, women ≥ 0.85) was 1.34 (1.16-1.55). There was an increased risk of cardiovascular disease (CVD) mortality associated with BMI-defined obesity, a high WC and a high WHR categories; the HR estimates for these were 1.36 (1.05-1.77), 1.41 (1.11-1.79) and 1.44 (1.12-1.85), respectively. A low BMI (<18.5 kg m(-2)) was associated with elevated HR for all-cause mortality (2.66; 1.97-3.60), for chronic respiratory disease mortality (3.17; 1.39-7.21) and for acute respiratory disease mortality (11.68; 5.01-27.21). This pattern was repeated for WC but not for WHR.
It might be prudent not to use BMI as the sole measure to summarize body size. The alternatives WC and WHR may more clearly define the health risks associated with excess body fat accumulation. The lack of association between elevated BMI and mortality may reflect the secular decline in CVD mortality.
探讨体重指数(BMI)、腰围(WC)或腰臀比(WHR)与全因死亡率或死因特异性死亡率之间的关系。
与住院和死亡记录相关的横断面调查。
来自苏格兰人群全国代表性样本的 20117 名成年人(年龄 18-86 岁)。
使用 Cox 比例风险模型估计全因或死因特异性死亡率的风险比(HR)。BMI、WC 和 WHR 这三个人体测量指标是主要关注的变量。调整变量包括年龄、性别、吸烟状况、饮酒量、调查年份、社会阶层和贫困地区。
BMI 定义的肥胖症(≥30kg/m²)与死亡率增加无关(HR=0.93;95%置信区间=0.80-1.08),而超重类别(25-<30kg/m²)与死亡率降低相关(0.80;0.70-0.91)。相比之下,高 WC(男性≥102cm,女性≥88cm)的 HR 为 1.17(1.02-1.34),高 WHR(男性≥1,女性≥0.85)的 HR 为 1.34(1.16-1.55)。与 BMI 定义的肥胖症、高 WC 和高 WHR 类别相关的心血管疾病(CVD)死亡率增加;这些 HR 估计值分别为 1.36(1.05-1.77)、1.41(1.11-1.79)和 1.44(1.12-1.85)。低 BMI(<18.5kg/m²)与全因死亡率(2.66;1.97-3.60)、慢性呼吸道疾病死亡率(3.17;1.39-7.21)和急性呼吸道疾病死亡率(11.68;5.01-27.21)升高的 HR 相关。这种模式在 WC 中重复出现,但在 WHR 中没有重复。
明智的做法可能是不要仅使用 BMI 作为总结身体大小的唯一指标。WC 和 WHR 等替代方法可能更清楚地定义与体脂肪过度积累相关的健康风险。BMI 升高与死亡率之间缺乏关联可能反映了 CVD 死亡率的长期下降。