Case Western Reserve University School of Medicine, Cleveland, OH, USA.
Respir Res. 2010 Oct 6;11(1):137. doi: 10.1186/1465-9921-11-137.
Cystic Fibrosis (CF) is a life-shortening genetic disease in which ~80% of deaths result from loss of lung function linked to inflammation due to chronic bacterial infection (principally Pseudomonas aeruginosa). Pulmonary exacerbations (intermittent episodes during which symptoms of lung infection increase and lung function decreases) can cause substantial resource utilization, morbidity, and irreversible loss of lung function. Intravenous antibiotic treatment to reduce exacerbation symptoms is standard management practice. However, no prospective studies have identified an optimal antibiotic treatment duration and this lack of objective data has been identified as an area of concern and interest.
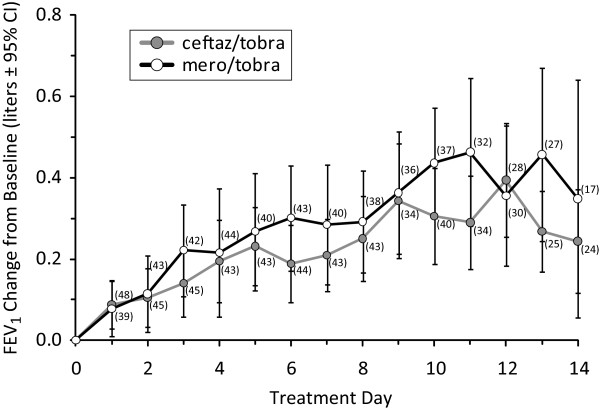
We have retrospectively analyzed pulmonary function response data (as forced expiratory volume in one second; FEV1) from a previous blinded controlled CF exacerbation management study of intravenous ceftazidime/tobramycin and meropenem/tobramycin in which spirometry was conducted daily to assess the time course of pulmonary function response.
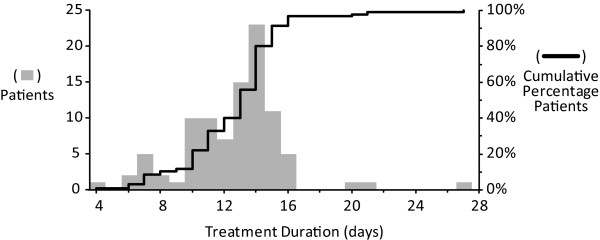
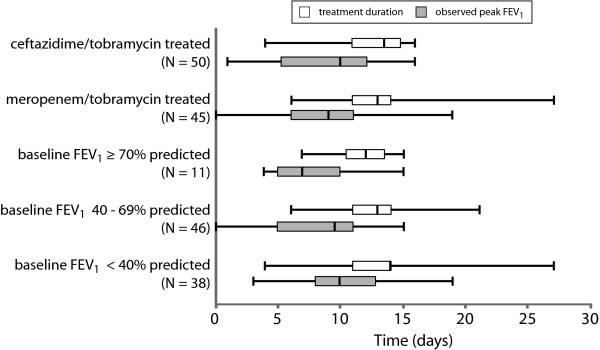
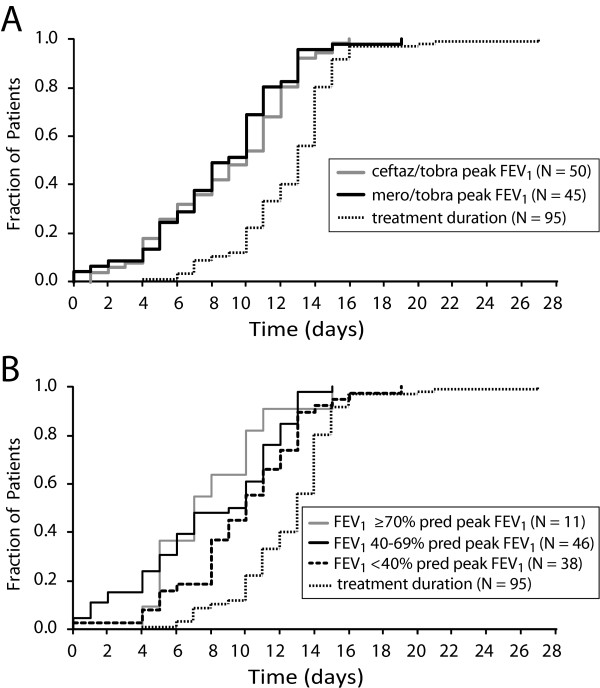
Ninety-five patients in the study received antibiotics for at least 4 days and were included in our analyses. Patients received antibiotics for an average of 12.6 days (median = 13, SD = 3.2 days), with a range of 4 to 27 days. No significant differences were observed in mean or median treatment durations as functions of either treatment group or baseline lung disease stage. Average time from initiation of antibiotic treatment to highest observed FEV1 was 8.7 days (median = 10, SD = 4.0 days), with a range of zero to 19 days. Patients were treated an average of 3.9 days beyond the day of peak FEV1 (median = 3, SD = 3.8 days), with 89 patients (93.7%) experiencing their peak FEV1 improvement within 13 days. There were no differences in mean or median times to peak FEV1 as a function of treatment group, although the magnitude of FEV1 improvement differed between groups.
Our results suggest that antibiotic response to exacerbation as assessed by pulmonary function is essentially complete within 2 weeks of treatment initiation and relatively independent of the magnitude of pulmonary function response observed.
囊性纤维化(CF)是一种缩短寿命的遗传性疾病,约 80%的死亡是由于肺部功能丧失导致的,这与慢性细菌感染(主要是铜绿假单胞菌)引起的炎症有关。肺部恶化(症状加重、肺部功能下降的间歇性发作)会导致大量资源的利用、发病率和不可逆转的肺部功能丧失。静脉内抗生素治疗以减轻恶化症状是标准的管理实践。然而,没有前瞻性研究确定了最佳的抗生素治疗持续时间,缺乏客观数据被认为是一个令人关注和感兴趣的领域。
我们回顾性分析了先前一项静脉内头孢他啶/妥布霉素和美罗培南/妥布霉素治疗 CF 恶化管理的盲法对照研究中的肺功能反应数据(作为一秒用力呼气量;FEV1),其中每天进行肺活量测定以评估肺功能反应的时间过程。
研究中 95 例患者至少接受了 4 天的抗生素治疗,并纳入了我们的分析。患者接受抗生素治疗的平均时间为 12.6 天(中位数=13,SD=3.2 天),范围为 4 至 27 天。在治疗组或基线肺部疾病阶段方面,治疗持续时间的平均值或中位数没有明显差异。从开始抗生素治疗到观察到的最高 FEV1 的平均时间为 8.7 天(中位数=10,SD=4.0 天),范围为零至 19 天。患者平均在达到 FEV1 峰值后再治疗 3.9 天(中位数=3,SD=3.8 天),89 例患者(93.7%)在 13 天内达到了 FEV1 的峰值改善。作为治疗组的函数,FEV1 达到峰值的平均或中位数时间没有差异,尽管两组之间的 FEV1 改善程度不同。
我们的结果表明,通过肺功能评估的恶化抗生素反应在治疗开始后 2 周内基本完成,并且相对独立于观察到的肺功能反应的程度。