Beuran Mircea, Nego Ionuţ, Ispas Alexandru Teodor, Păun Softin, Runcanu Alexandru, Lupu Giorgica, Venter Dan
Section Surgery, Emergency Hospital, Bucharest, Romania 8 Calea Floreasca, District 1, Bucharest, 014461, Romania.
J Med Life. 2010 Jul-Sep;3(3):289-96.
Nonoperative management (NOM) of liver trauma is currently rather the rule than the exception. However, the current evidence presents subgroups of patients at higher risk for NOM failure. These patients must be treated more cautiously regarding the NOM approach.
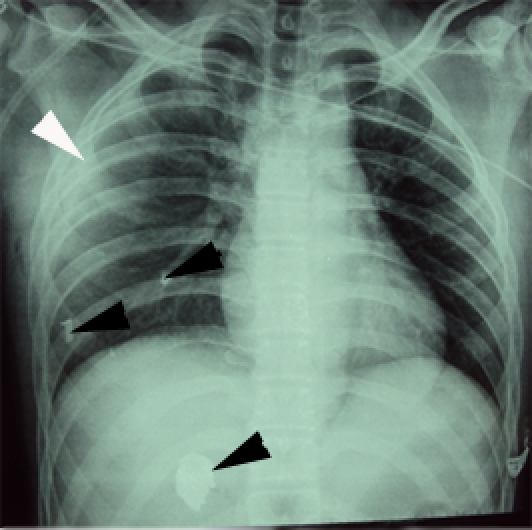
A case report of 3 polytrauma patients (Injury Severity Score > 17) with high-degree liver trauma managed nonoperatively.
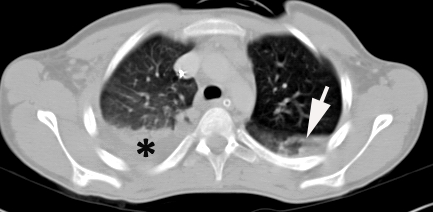
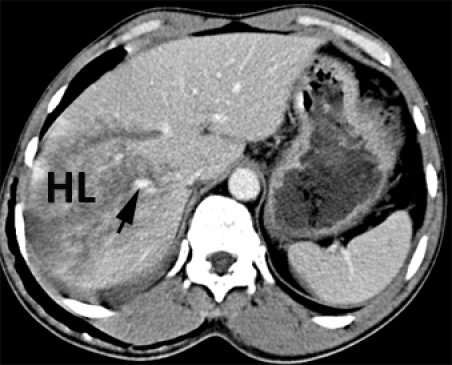
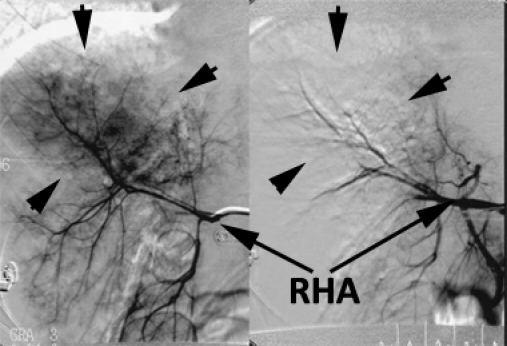
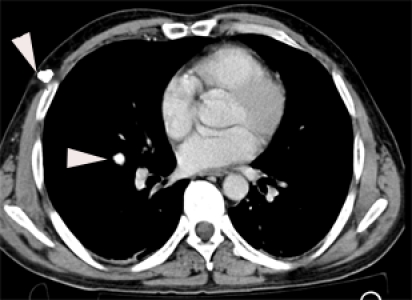
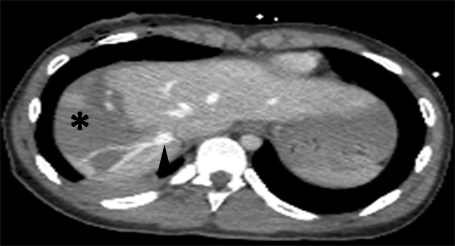
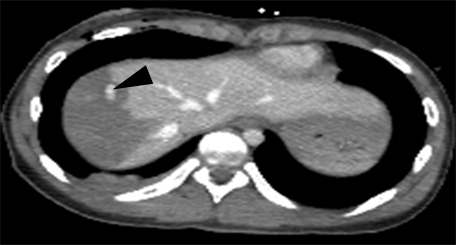
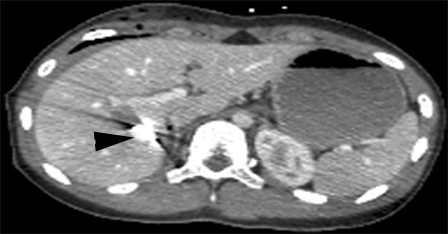
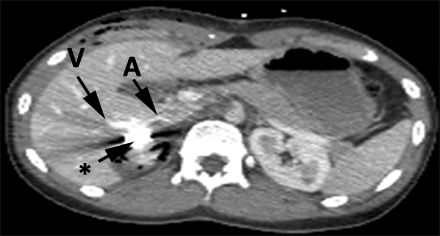
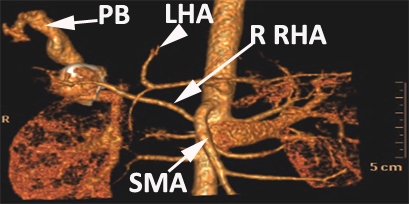
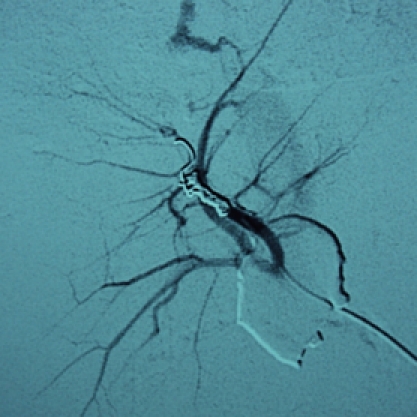
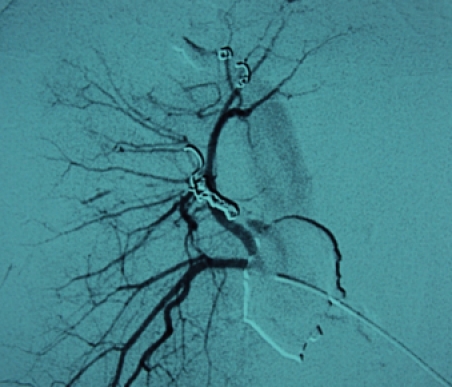
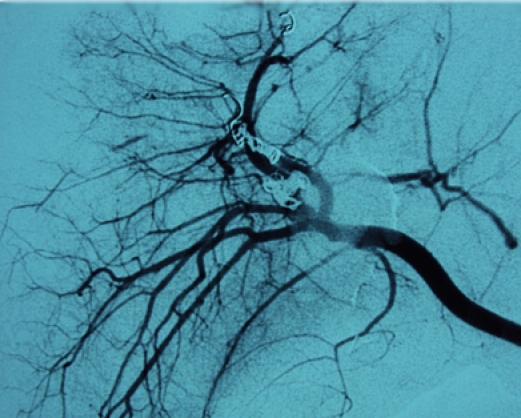
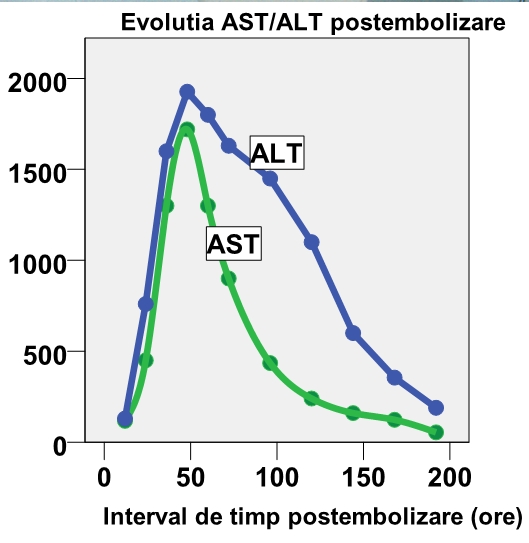
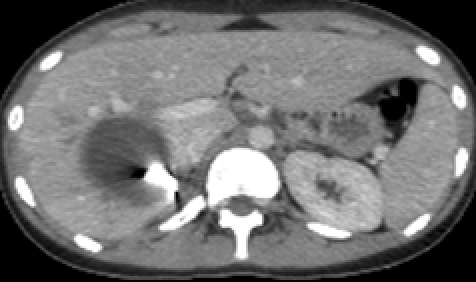
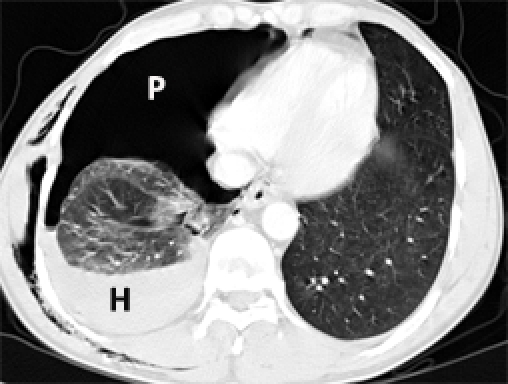
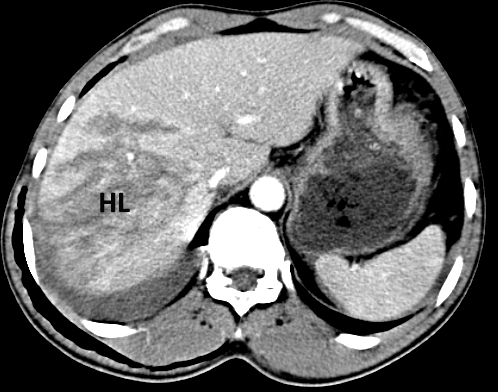
The first case presented is the one of a polytrauma patient with degree IV liver injury and impaired mental status. It was a high risk for NOM failure because there was an angiographically hemostasis. The second case is one of a polytrauma patient who became hemodynamically stable after the administration of 2000 ml of fluid intravenously. There was a nonoperative approach with angiography and embolization of degree IV liver injury. Despite the success of the nonoperative treatment, there was an important hepatic necrosis following embolization. The third case is one of a polytrauma patient with a degree IV hepatic injury. Success was accomplished in NOM without an angiography.
Nonoperative management of liver injuries can be applied safely even in high degree hepatic trauma. In hemodynamically metastable patients or impaired mental status patients, the nonoperative approach can be applied successfully, but the trauma surgeon must be very cautious.
目前,肝外伤的非手术治疗(NOM)已相当普遍,而非个别情况。然而,现有证据表明存在NOM失败风险较高的患者亚组。对于这些患者,在采用NOM方法时必须更加谨慎。
报告3例多发伤患者(损伤严重度评分>17)伴有严重肝外伤且采用非手术治疗的病例。
首例病例是一名多发伤患者,肝脏损伤为IV级且意识状态受损。由于血管造影显示有止血情况,该病例NOM失败风险较高。第二例病例是一名多发伤患者,静脉输注2000毫升液体后血流动力学稳定。对IV级肝损伤采用血管造影和栓塞的非手术方法。尽管非手术治疗成功,但栓塞后出现了重要的肝坏死。第三例病例是一名多发伤患者,肝脏损伤为IV级。未进行血管造影的NOM取得了成功。
即使在严重肝外伤中,肝损伤的非手术治疗也可安全应用。对于血流动力学稳定或意识状态受损的患者,非手术方法可成功应用,但创伤外科医生必须非常谨慎。