Division of Cardiology, CV MRI Center, Allegheny General Hospital, Pittsburgh, Pennsylvania 15212-4772, USA.
JACC Cardiovasc Imaging. 2010 Oct;3(10):1030-6. doi: 10.1016/j.jcmg.2010.07.008.
The purpose of this study was to assess the prognostic value of global magnetic resonance (MR) myocardial perfusion imaging (MPI) in women with suspected myocardial ischemia and no obstructive (stenosis <50%) coronary artery disease (CAD).
The prognostic value of global MR-MPI in women without obstructive CAD remains unknown.
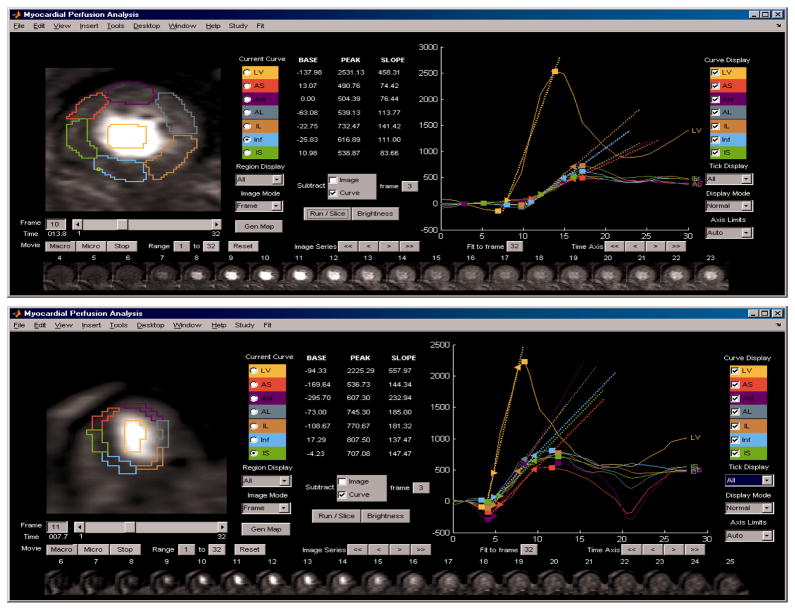
Women (n = 100, mean age 57 ± 11 years, age range 31 to 76 years), with symptoms of myocardial ischemia and with no obstructive CAD, as assessed by coronary angiography, underwent MR-MPI and standard functional assessment. During follow-up (34 ± 16 months), time to first adverse event (death, myocardial infarction, or hospitalization for worsening anginal symptoms) was analyzed using global MPI and left ventricular ejection fraction (EF) data.
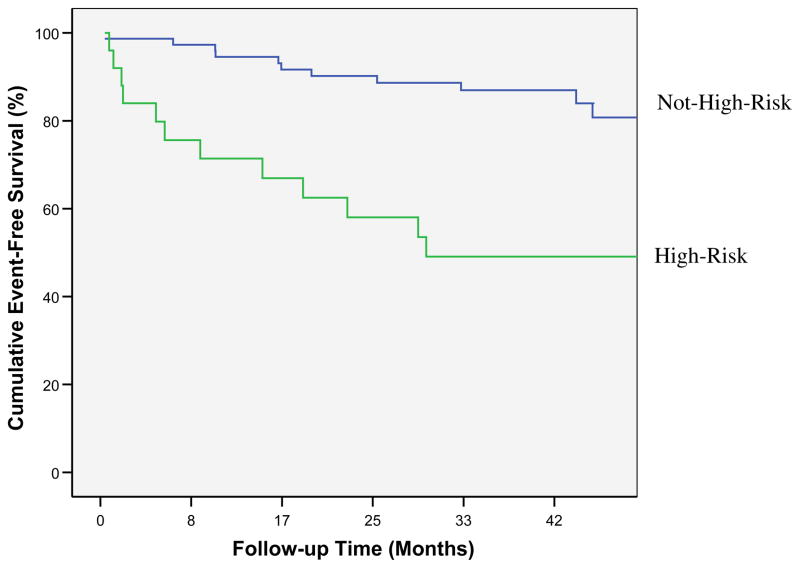
Adverse events occurred in 23 (23%) women. Using univariable Cox proportional hazards regression modeling, variables found to be predictive of adverse events were global MR-MPI average uptake slope (p < 0.05), the ratio of MR-MPI peak signal amplitude to uptake slope (p < 0.05), and EF (p < 0.05). Two multivariable Cox models were formed, 1 using variables that were performance site dependent: ratio of MR-MPI peak amplitude to uptake slope together with EF (chi square: 13, p < 0.005); and a model using variables that were performance site independent: MR-MPI slope and EF (chi square: 12, p < 0.005). Each of the 2 multivariable models remained predictive of adverse events after adjustment for age, disease history, and Framingham risk score. For each of the Cox models, patients were categorized as high risk if they were in the upper quartile of the model and as not high risk otherwise. Kaplan-Meier analysis of time to event was performed for high risk versus not high risk for site-dependent (log rank: 15.2, p < 0.001) and site-independent (log rank: 13.0, p < 001) models.
Among women with suspected myocardial ischemia and no obstructive CAD, MR-MPI-determined global measurements of normalized uptake slope and peak signal uptake, together with global functional assessment of EF, appear to predict prognosis.
本研究旨在评估全球磁共振(MR)心肌灌注成像(MPI)在疑似心肌缺血且无阻塞性(狭窄<50%)冠状动脉疾病(CAD)的女性中的预后价值。
全球 MR-MPI 在无阻塞性 CAD 的女性中的预后价值尚不清楚。
100 名女性(平均年龄 57±11 岁,年龄范围 31 至 76 岁),有心肌缺血症状,且冠状动脉造影检查无阻塞性 CAD,进行了 MR-MPI 和标准功能评估。在随访期间(34±16 个月),使用全球 MPI 和左心室射血分数(EF)数据分析首次不良事件(死亡、心肌梗死或因恶化的心绞痛症状而住院)的时间。
23 名(23%)女性发生不良事件。使用单变量 Cox 比例风险回归模型,发现可预测不良事件的变量包括全球 MR-MPI 平均摄取斜率(p<0.05)、MR-MPI 峰值信号幅度与摄取斜率的比值(p<0.05)和 EF(p<0.05)。建立了 2 个多变量 Cox 模型,1 个模型使用与性能站点相关的变量:MR-MPI 峰值幅度与摄取斜率的比值与 EF 一起(卡方:13,p<0.005);另一个模型使用与性能站点无关的变量:MR-MPI 斜率和 EF(卡方:12,p<0.005)。在调整年龄、病史和 Framingham 风险评分后,每个多变量模型仍然可预测不良事件。对于每个 Cox 模型,如果患者处于模型的上四分位数,则将其归类为高危,否则为非高危。对依赖站点(对数秩:15.2,p<0.001)和独立站点(对数秩:13.0,p<0.001)模型进行高风险与非高风险的 Kaplan-Meier 时间事件分析。
在疑似心肌缺血且无阻塞性 CAD 的女性中,MR-MPI 确定的正常摄取斜率和峰值信号摄取的全球测量值,以及 EF 的全球功能评估,似乎可以预测预后。