Critical Care and Trauma Division, The George Institute for International Health, PO Box M201, Missenden Road, NSW 2050, Australia.
Crit Care. 2010;14(5):R185. doi: 10.1186/cc9293. Epub 2010 Oct 15.
Recent evidence suggests that choice of fluid used for resuscitation may influence mortality in critically ill patients.
We conducted a cross-sectional study in 391 intensive care units across 25 countries to describe the types of fluids administered during resuscitation episodes. We used generalized estimating equations to examine the association between patient, prescriber and geographic factors and the type of fluid administered (classified as crystalloid, colloid or blood products).
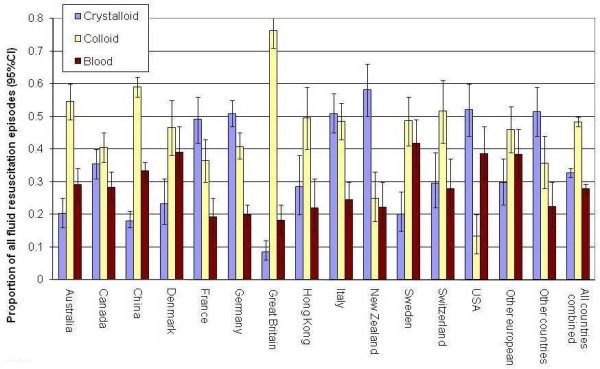
During the 24-hour study period, 1,955 of 5,274 (37.1%) patients received resuscitation fluid during 4,488 resuscitation episodes. The main indications for administering crystalloid or colloid were impaired perfusion (1,526/3,419 (44.6%) of episodes), or to correct abnormal vital signs (1,189/3,419 (34.8%)). Overall, colloid was administered to more patients (1,234 (23.4%) versus 782 (14.8%)) and during more episodes (2,173 (48.4%) versus 1,468 (32.7%)) than crystalloid. After adjusting for patient and prescriber characteristics, practice varied significantly between countries with country being a strong independent determinant of the type of fluid prescribed. Compared to Canada where crystalloid, colloid and blood products were administered in 35.5%, 40.6% and 28.3% of resuscitation episodes respectively, odds ratios for the prescription of crystalloid in China, Great Britain and New Zealand were 0.46 (95% confidence interval (CI) 0.30 to 0.69), 0.18 (0.10 to 0.32) and 3.43 (1.71 to 6.84) respectively; odds ratios for the prescription of colloid in China, Great Britain and New Zealand were 1.72 (1.20 to 2.47), 4.72 (2.99 to 7.44) and 0.39 (0.21 to 0.74) respectively. In contrast, choice of fluid was not influenced by measures of illness severity (for example, Acute Physiology and Chronic Health Evaluation (APACHE) II score).
Administration of resuscitation fluid is a common intervention in intensive care units and choice of fluid varies markedly between countries. Although colloid solutions are more expensive and may possibly be harmful in some patients, they were administered to more patients and during more resuscitation episodes than crystalloids were.
最近的证据表明,复苏时选择的液体可能会影响危重症患者的死亡率。
我们在 25 个国家的 391 个重症监护病房进行了一项横断面研究,以描述复苏期间使用的液体类型。我们使用广义估计方程来检查患者、处方者和地理因素与所使用的液体类型(分为晶体液、胶体液或血制品)之间的关联。
在 24 小时的研究期间,5274 例患者中有 1955 例(37.1%)在 4488 例复苏中接受了复苏液。给予晶体液或胶体液的主要指征是灌注受损(1526/3419[44.6%])或纠正异常生命体征(1189/3419[34.8%])。总体而言,胶体液的使用量更大(1234 例[23.4%]比 782 例[14.8%]),使用的复苏次数也更多(2173 例[48.4%]比 1468 例[32.7%])。在调整了患者和处方者特征后,各国之间的实践差异很大,国家是处方类型的重要独立决定因素。与加拿大相比,在加拿大,晶体液、胶体液和血制品分别在 35.5%、40.6%和 28.3%的复苏中使用,中国、英国和新西兰晶体液处方的比值比分别为 0.46(95%置信区间为 0.30 至 0.69)、0.18(0.10 至 0.32)和 3.43(1.71 至 6.84);中国、英国和新西兰胶体液处方的比值比分别为 1.72(1.20 至 2.47)、4.72(2.99 至 7.44)和 0.39(0.21 至 0.74)。相比之下,液体的选择不受疾病严重程度的衡量标准(例如,急性生理学和慢性健康评估(APACHE)Ⅱ评分)的影响。
复苏液的使用是重症监护病房的常见干预措施,各国之间的液体选择差异很大。尽管胶体溶液更昂贵,并且在某些患者中可能有害,但它们在更多的患者中使用,并且在更多的复苏中使用,而不是晶体液。