Division of Nuclear Medicine, Department of Imaging, Cedars-Sinai Medical Center, Los Angeles, California 90048, USA.
J Nucl Med. 2010 Nov;51(11):1724-31. doi: 10.2967/jnumed.110.078782. Epub 2010 Oct 18.
A recently developed camera system for high-speed SPECT (HS-SPECT) myocardial perfusion imaging shows excellent correlation with conventional SPECT. Our goal was to test the diagnostic accuracy of an automated quantification of combined upright and supine myocardial SPECT for detection of coronary artery disease (CAD) (≥ 70% luminal diameter stenosis or, in left main coronary artery, ≥ 50% luminal diameter stenosis) in comparison to invasive coronary angiography (ICA).
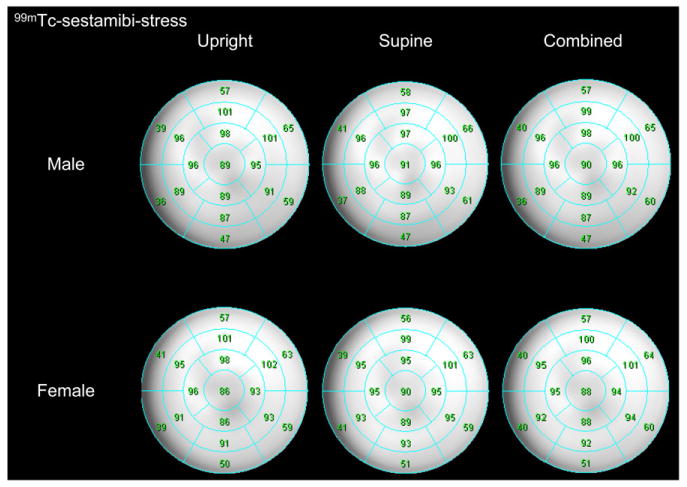
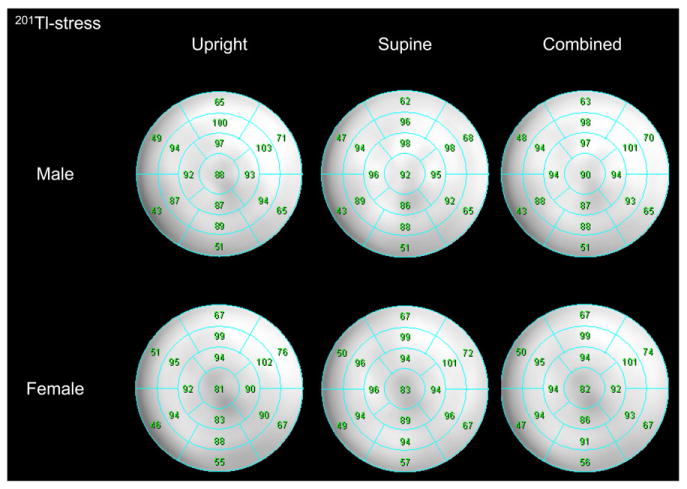
We studied 142 patients undergoing upright and supine HS-SPECT, including 56 consecutive patients (63% men; mean age ± SD, 64 ± 13 y; 45% exercise stress) without known CAD who underwent diagnostic ICA within 6 mo of HS-SPECT and 86 consecutive patients with a low likelihood of CAD. Reference limits for upright and supine HS-SPECT were created from studies of patients with a low likelihood of CAD. Automated software adopted from supine-prone analysis was used to quantify the severity and extent of perfusion abnormality and was expressed as total perfusion deficit (TPD). TPD was obtained for upright (U-TPD), supine (S-TPD), and combined upright-supine acquisitions (C-TPD). Stress U-TPD ≥ 5%, S-TPD ≥ 5%, and C-TPD ≥ 3% myocardium were considered abnormal for per-patient analysis, and U-TPD, S-TPD, and C-TPD ≥ 2% in each coronary artery territory were considered abnormal for per-vessel analysis.
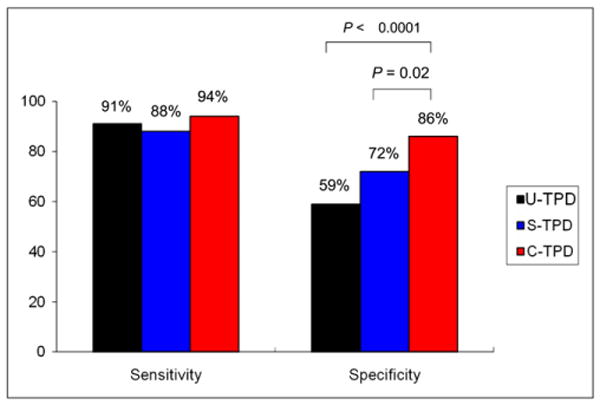
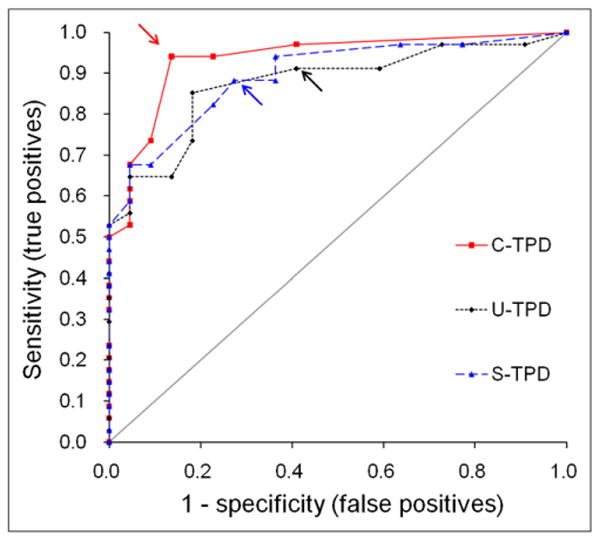
On a per-patient basis, the sensitivity was 91%, 88%, and 94% for U-TPD, S-TPD, and C-TPD, respectively, and specificity was 59%, 73%, and 86% for U-TPD, S-TPD, and C-TPD, respectively. C-TPD had a larger area under the receiver-operating-characteristic curve than U-TPD or S-TPD for identification of stenosis ≥ 70% (0.94 vs. 0.88 and 0.89, P < 0.05 and not significant, respectively). On a per-vessel basis, the sensitivity was 67%, 66%, and 69% for U-TPD, S-TPD, and C-TPD, respectively, and specificity was 91%, 94%, and 97% for U-TPD, S-TPD, and C-TPD, respectively (P = 0.02 for specificity U-TPD vs. C-TPD).
In this first comparison of HS-SPECT with ICA, new automated quantification of combined upright and supine HS-SPECT shows high diagnostic accuracy for detecting clinically significant CAD, with findings comparable to those reported using conventional SPECT.
本研究旨在比较新型高帧率单光子发射型计算机断层扫描(HS-SPECT)心肌灌注显像与有创冠状动脉造影(ICA)对检测冠状动脉疾病(CAD)(管腔直径狭窄≥70%,或左主干 CAD 管腔直径狭窄≥50%)的诊断准确性,该系统是最近开发的一种用于 HS-SPECT 心肌灌注成像的相机系统,与常规 SPECT 具有极好的相关性。
我们对 142 例行直立位和仰卧位 HS-SPECT 的患者进行了研究,包括 56 例连续患者(63%为男性;平均年龄±标准差,64±13 岁;45%为运动负荷),这些患者在 HS-SPECT 后 6 个月内行 ICA 检查,且无已知 CAD。来自低 CAD 可能性患者的研究中创建了直立位和仰卧位 HS-SPECT 的参考限值。采用来自仰卧位-俯卧位分析的自动软件定量评估灌注异常的严重程度和范围,并表示为总灌注缺损(TPD)。为每位患者获得直立位(U-TPD)、仰卧位(S-TPD)和直立位-仰卧位联合采集(C-TPD)的 TPD。将每位患者的 U-TPD >5%、S-TPD >5%和 C-TPD >3%视为异常,每支冠状动脉的 U-TPD、S-TPD 和 C-TPD >2%视为异常。
以每位患者为基础,U-TPD、S-TPD 和 C-TPD 的敏感性分别为 91%、88%和 94%,特异性分别为 59%、73%和 86%。对于识别狭窄≥70%的病变,C-TPD 的受试者工作特征曲线下面积大于 U-TPD 或 S-TPD(0.94 比 0.88 和 0.89,P<0.05 和无显著差异)。以每支血管为基础,U-TPD、S-TPD 和 C-TPD 的敏感性分别为 67%、66%和 69%,特异性分别为 91%、94%和 97%(U-TPD 与 C-TPD 之间的特异性具有统计学差异,P=0.02)。
在这项与 ICA 的首次比较研究中,新型直立位和仰卧位 HS-SPECT 的新自动定量分析显示出检测有临床意义 CAD 的高诊断准确性,其结果与使用常规 SPECT 报道的结果相当。