Michigan State University, International Neurologic and Psychiatric Epidemiology Program, East Lansing, MI, USA.
Malawi-Liverpool-Wellcome Trust Clinical Research Programme, College of Medicine, Malawi, and The Liverpool School of Tropical Medicine, University of Liverpool, Liverpool, UK.
Lancet Neurol. 2010 Dec;9(12):1173-1181. doi: 10.1016/S1474-4422(10)70270-2. Epub 2010 Nov 4.
Cerebral malaria, a disorder characterised by coma, parasitaemia, and no other evident cause of coma, is challenging to diagnose definitively in endemic regions that have high rates of asymptomatic parasitaemia and limited neurodiagnostic facilities. A recently described malaria retinopathy improves diagnostic specificity. We aimed to establish whether retinopathy-positive cerebral malaria is a risk factor for epilepsy or other neurodisabilities.
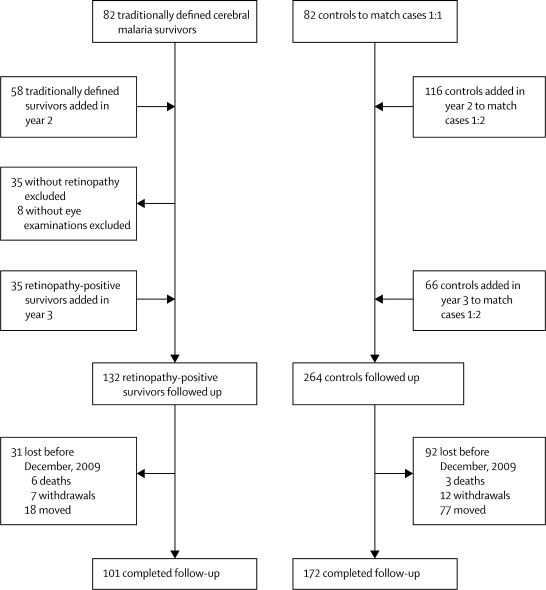
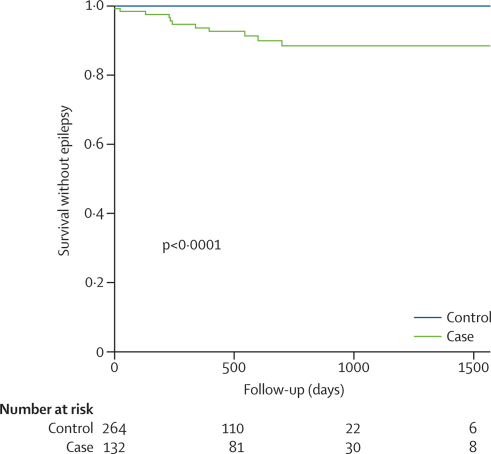
Between 2005 and 2007, we did a prospective cohort study of survivors of cerebral malaria with malaria retinopathy in Blantyre, Malawi. Children with cerebral malaria were identified at the time of their index admission and age-matched to concurrently admitted children without coma or nervous system infection. Initially matching of cases to controls was 1:1 but, in 2006, enrolment criteria for cerebral malaria survivors were revised to limit inclusion to children with cerebral malaria and retinopathy on the basis of indirect ophthalmoscopic examination; matching was then changed to 1:2 and the revised inclusion criteria were applied retrospectively for children enrolled previously. Clinical assessments at discharge and standardised nurse-led follow-up every 3 months thereafter were done to identify children with new seizure disorders or other neurodisabilities. A Kaplan-Meier survival analysis was done for incident epilepsy.
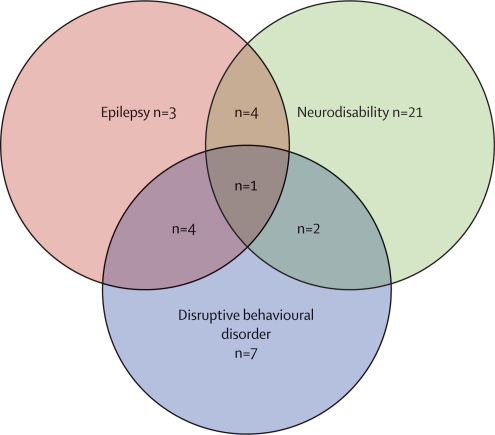
132 children with retinopathy-positive cerebral malaria and 264 age-matched, non-comatose controls were followed up for a median of 495 days (IQR 195-819). 12 of 132 cerebral malaria survivors developed epilepsy versus none of 264 controls (odds ratio [OR] undefined; p<0·0001). 28 of 121 cerebral malaria survivors developed new neurodisabilities, characterised by gross motor, sensory, or language deficits, compared with two of 253 controls (OR 37·8, 95% CI 8·8-161·8; p<0·0001). The risk factors for epilepsy in children with cerebral malaria were a higher maximum temperature (39·4°C [SD 1·2] vs 38·5°C [1·1]; p=0·01) and acute seizures (11/12 vs 76/120; OR 6·37, 95% CI 1·02-141·2), and male sex was a risk factor for new neurodisabilities (20/28 vs 38/93; OR 3·62, 1·44-9·06).
Almost a third of retinopathy-positive cerebral malaria survivors developed epilepsy or other neurobehavioural sequelae. Neuroprotective clinical trials aimed at managing hyperpyrexia and optimising seizure control are warranted.
US National Institutes of Health and Wellcome Trust.
脑型疟疾是一种以昏迷、寄生虫血症和无其他明显昏迷原因为特征的疾病,在寄生虫血症无症状率高且神经诊断设施有限的流行地区,其确诊具有挑战性。最近描述的疟疾性视网膜病变提高了诊断的特异性。我们旨在确定视网膜阳性脑型疟疾是否是癫痫或其他神经功能障碍的危险因素。
在 2005 年至 2007 年期间,我们在马拉维布兰太尔对患有脑型疟疾和疟疾性视网膜病变的幸存者进行了一项前瞻性队列研究。在入院时发现患有脑型疟疾的儿童,并与同时入院的无昏迷或神经系统感染的儿童进行年龄匹配。最初病例与对照的匹配比例为 1:1,但在 2006 年,对脑型疟疾幸存者的纳入标准进行了修订,以限制仅包括根据间接眼底检查患有脑型疟疾和视网膜病变的儿童;随后改为 1:2,并对之前入组的儿童进行了回溯性应用修订后的纳入标准。在出院时进行临床评估,并在之后每 3 个月由标准化护士进行随访,以确定是否有新的癫痫发作或其他神经功能障碍。对新发癫痫进行 Kaplan-Meier 生存分析。
132 名患有视网膜阳性脑型疟疾的儿童和 264 名年龄匹配、非昏迷对照者接受了中位数为 495 天(IQR 195-819)的随访。在 132 名脑型疟疾幸存者中,有 12 名发展为癫痫,而在 264 名对照者中无一例(比值比[OR]未定义;p<0·0001)。在 121 名脑型疟疾幸存者中,有 28 名出现了新的神经功能障碍,表现为粗大运动、感觉或语言缺陷,而在 253 名对照者中只有 2 名(OR 37.8,95%CI 8.8-161.8;p<0·0001)。患有脑型疟疾的儿童发生癫痫的危险因素是更高的最高体温(39.4°C [SD 1.2] vs 38.5°C [1.1];p=0·01)和急性癫痫发作(11/12 例 vs 76/120 例;OR 6.37,95%CI 1.02-141.2),而男性是新发神经功能障碍的危险因素(20/28 例 vs 38/93 例;OR 3.62,1.44-9.06)。
近三分之一的视网膜阳性脑型疟疾幸存者出现癫痫或其他神经行为后遗症。有必要进行神经保护临床试验,以管理高热和优化癫痫发作控制。
美国国立卫生研究院和惠康信托基金会。