Department of Cardiovascular Medicine, University of Oxford, John Radcliffe Hospital, UK.
J Cardiovasc Magn Reson. 2010 Nov 16;12(1):66. doi: 10.1186/1532-429X-12-66.
Adenosine is the most widely used vasodilator stress agent for cardiovascular magnetic resonance (CMR) perfusion studies. With the standard dose of 140 mcg/kg/min some patients fail to demonstrate characteristic haemodynamic changes: a significant increase in heart rate (HR) and mild decrease in systolic blood pressure (SBP). Whether an increase in the rate of adenosine infusion would improve peripheral and, likely, coronary vasodilatation in those patients is unknown. The aim of the present study was to assess the tolerance and safety of a high-dose adenosine protocol in patients with inadequate haemodynamic response to the standard adenosine protocol when undergoing CMR perfusion imaging.
98 consecutive patients with known or suspected coronary artery disease (CAD) underwent CMR perfusion imaging at 1.5 Tesla. Subjects were screened for contraindications to adenosine, and an electrocardiogram was performed prior to the scan. All patients initially received the standard adenosine protocol (140 mcg/kg/min for at least 3 minutes). If the haemodynamic response was inadequate (HR increase < 10 bpm or SBP decrease < 10 mmHg) then the infusion rate was increased up to a maximum of 210 mcg/kg/min (maximal infusion duration 7 minutes).
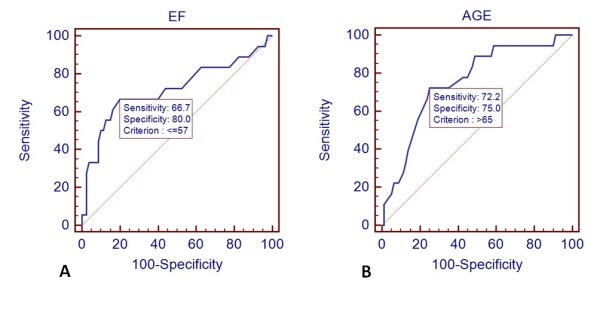
All patients successfully completed the CMR scan. Of a total of 98 patients, 18 (18%) did not demonstrate evidence of a significant increase in HR or decrease in SBP under the standard adenosine infusion rate. Following the increase in the rate of infusion, 16 out of those 18 patients showed an adequate haemodynamic response. One patient of the standard infusion group and two patients of the high-dose group developed transient advanced AV block. Significantly more patients complained of chest pain in the high-dose group (61% vs. 29%, p = 0.009). On multivariate analysis, age > 65 years and ejection fraction < 57% were the only independent predictors of blunted haemodynamic responsiveness to adenosine.
A substantial number of patients do not show adequate peripheral haemodynamic response to standard-dose adenosine stress during perfusion CMR imaging. Age and reduced ejection fraction are predictors of inadequate response to standard dose adenosine. A high-dose adenosine protocol (up to 210 mcg/kg/min) is well tolerated and results in adequate haemodynamic response in nearly all patients.
腺苷是心血管磁共振(CMR)灌注研究中最广泛使用的血管扩张剂应激剂。在标准剂量为 140mcg/kg/min 的情况下,一些患者未能表现出特征性的血液动力学变化:心率(HR)显著增加,收缩压(SBP)轻度下降。在那些患者中,增加腺苷输注速率是否会改善外周和可能的冠状动脉扩张尚不清楚。本研究的目的是评估在接受 CMR 灌注成像时,标准腺苷方案血液动力学反应不足的患者中高剂量腺苷方案的耐受性和安全性。
98 例连续的已知或疑似冠状动脉疾病(CAD)患者在 1.5T 进行 CMR 灌注成像。对患者进行腺苷禁忌证筛查,并在扫描前进行心电图检查。所有患者最初均接受标准腺苷方案(至少 3 分钟 140mcg/kg/min)。如果血液动力学反应不足(HR 增加<10bpm 或 SBP 下降<10mmHg),则将输注速率增加至最高 210mcg/kg/min(最大输注时间 7 分钟)。
所有患者均成功完成 CMR 扫描。在总共 98 例患者中,18 例(18%)在标准腺苷输注率下未显示 HR 显著增加或 SBP 下降的证据。在增加输注速率后,其中 18 例患者中有 16 例表现出适当的血液动力学反应。标准输注组的 1 例患者和高剂量组的 2 例患者出现短暂的高级房室传导阻滞。高剂量组有更多的患者诉胸痛(61%比 29%,p=0.009)。多变量分析显示,年龄>65 岁和射血分数<57%是腺苷血液动力学反应迟钝的唯一独立预测因素。
在灌注 CMR 成像期间,相当数量的患者对标准剂量的腺苷应激没有表现出足够的外周血液动力学反应。年龄和射血分数降低是对标准剂量腺苷反应不足的预测因素。高剂量腺苷方案(高达 210mcg/kg/min)具有良好的耐受性,并使几乎所有患者都能获得充分的血液动力学反应。