Division of Health System, Policy and Management, School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong.
BMC Health Serv Res. 2010 Nov 17;10:311. doi: 10.1186/1472-6963-10-311.
Studies that identify reasons for readmissions are gaining importance in the light of the changing demographics worldwide which has led to greater demand for hospital beds. It is essential to profile the prevalence of avoidable readmissions and understand its drivers so as to develop possible interventions for reducing readmissions that are preventable. The aim of this study is to identify the magnitude of avoidable readmissions, its contributing factors and costs in Hong Kong.
This was a retrospective analysis of 332,453 inpatient admissions in the Medical specialty in public hospital system in Hong Kong in year 2007. A stratified random sample of patients with unplanned readmission within 30 days after discharge was selected for medical record reviews. Eight physicians reviewed patients' medical records and classified whether a readmission was avoidable according to an assessment checklist. The results were correlated with hospital inpatient data.
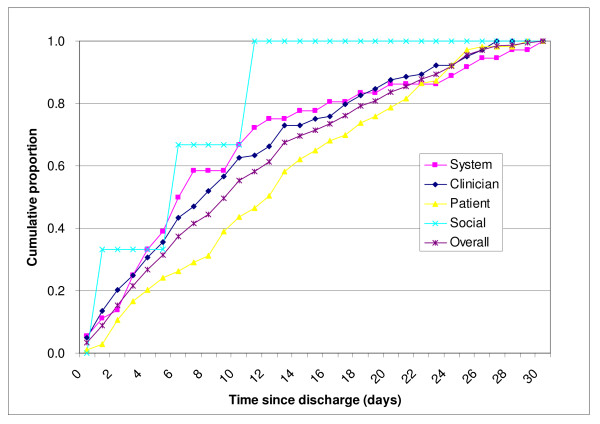
It was found that 40.8% of the 603 unplanned readmissions were judged avoidable by the reviewers. Avoidable readmissions were due to: clinician factor (42.3%) including low threshold for admission and premature discharge etc.; patient factor (including medical and health factor) (41.9%) such as relapse or progress of previous complaint, and compliance problems etc., followed by system factor (14.6%) including inadequate discharge planning, inadequate palliative care/terminal care, etc., and social factor (1.2%) such as carer system, lack of support and community services. After adjusting for patients' age, gender, principal diagnosis at previous discharge and readmission hospitals, the risk factors for avoidable readmissions in the total population i.e. all acute care admissions irrespective of whether there was a readmission or not, included patients with a longer length of stay, and with higher number of hospitalizations and attendance in public outpatient clinics and Accident and Emergency departments in the past 12 months. In the analysis of only unplanned readmissions, it was found that the concordance of the principal diagnosis for admission and readmission, and shorter time period between discharge and readmission were associated with avoidable readmissions.
Our study found that almost half of the readmissions could have been prevented. They had been mainly due to clinician and patient factors, in particular, both of which were intimately related to clinical management and patient care. These readmissions could be prevented by a system of ongoing clinical review to examine the clinical practice/decision for discharge, and improving clinical care and enhancing patient knowledge of the early warning signs for relapse. The importance of adequate and appropriate ambulatory care to support the patients in the community was also a key finding to reduce avoidable readmissions. Education on patient self-management should also be enhanced to minimize the patient factors with regard to avoidable readmission. Our findings thus provide important insights into the development of an effective discharge planning system which should place patients and carers as the primacy focus of care by engaging them along with the healthcare professionals in the whole discharge planning process.
随着全球人口结构的变化,对医院床位的需求增加,识别再入院原因的研究变得越来越重要。对可避免再入院的发生率及其驱动因素进行分析,以制定可能的干预措施来减少可预防的再入院,这一点至关重要。本研究旨在确定香港可避免再入院的程度、其相关因素和成本。
这是对 2007 年香港公立医院系统内科住院患者 332453 例的回顾性分析。对出院后 30 天内计划外再入院的患者进行分层随机抽样,选择病历进行回顾。8 名医生对患者的病历进行审查,并根据评估检查表判断再入院是否可避免。结果与医院住院数据相关联。
研究发现,603 例计划外再入院中有 40.8%的再入院可由评审员判断为可避免。可避免的再入院原因如下:临床医生因素(42.3%),包括入院和过早出院的门槛低等;患者因素(包括医疗和健康因素)(41.9%),如先前投诉的复发或进展,以及遵医嘱问题等;其次是系统因素(14.6%),包括出院计划不充分、姑息治疗/临终关怀不足等;社会因素(1.2%),如照顾者系统、缺乏支持和社区服务等。在调整患者的年龄、性别、上次出院时的主要诊断和再入院医院后,无论是否有再入院,所有急性护理入院的总人口(即所有急性护理入院患者)的可避免再入院的风险因素包括住院时间更长,以及过去 12 个月内住院和就诊次数更多、在公共门诊和急症室就诊次数更多。在仅分析计划外再入院的研究中,发现入院和再入院的主要诊断一致性,以及出院和再入院之间的时间间隔较短,与可避免再入院有关。
我们的研究发现,近一半的再入院是可以预防的。它们主要是由于临床医生和患者的因素造成的,特别是这两个因素都与临床管理和患者护理密切相关。通过对出院临床实践/决策进行持续的临床审查,改善临床护理,增强患者对复发早期预警信号的认识,可预防这些再入院。充分和适当的门诊护理以支持社区中的患者也是减少可避免再入院的一个关键发现。还应加强对患者自我管理的教育,以尽量减少与可避免再入院相关的患者因素。因此,我们的研究结果为制定有效的出院计划系统提供了重要的见解,该系统应将患者及其照顾者作为护理的首要重点,让他们与医疗保健专业人员一起参与整个出院计划过程。