University of California, San Francisco, San Francisco, CA 94143-0116, USA.
N Engl J Med. 2010 Nov 18;363(21):2004-14. doi: 10.1056/NEJMoa1001197.
The outcomes of kidney transplantation and immunosuppression in people infected with human immunodeficiency virus (HIV) are incompletely understood.
We undertook a prospective, nonrandomized trial of kidney transplantation in HIV-infected candidates who had CD4+ T-cell counts of at least 200 per cubic millimeter and undetectable plasma HIV type 1 (HIV-1) RNA levels while being treated with a stable antiretroviral regimen. Post-transplantation management was provided in accordance with study protocols that defined prophylaxis against opportunistic infection, indications for biopsy, and acceptable approaches to immunosuppression, management of rejection, and antiretroviral therapy.
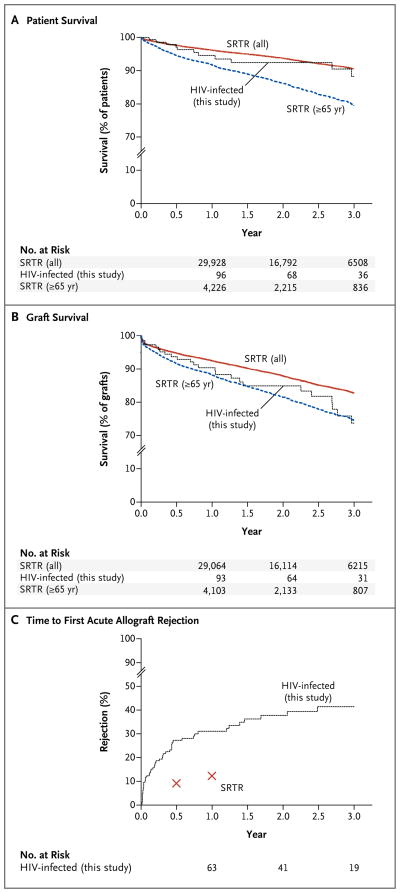
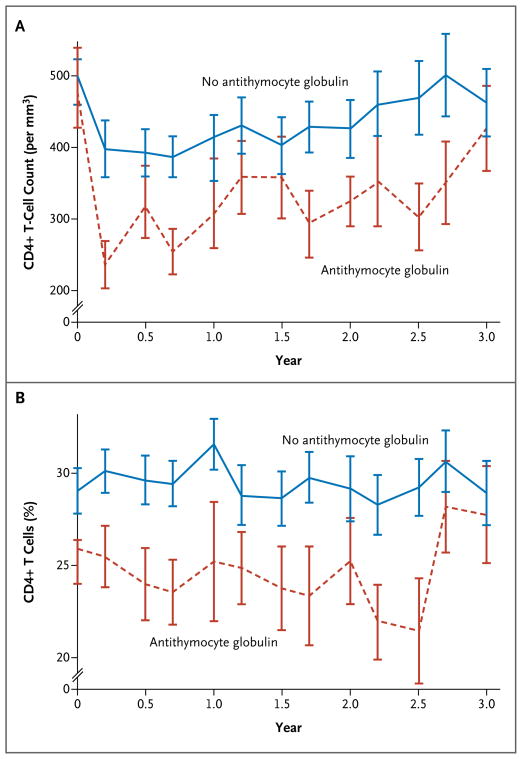
Between November 2003 and June 2009, a total of 150 patients underwent kidney transplantation; survivors were followed for a median period of 1.7 years. Patient survival rates (±SD) at 1 year and 3 years were 94.6±2.0% and 88.2±3.8%, respectively, and the corresponding mean graft-survival rates were 90.4% and 73.7%. In general, these rates fall somewhere between those reported in the national database for older kidney-transplant recipients (≥65 years) and those reported for all kidney-transplant recipients. A multivariate proportional-hazards analysis showed that the risk of graft loss was increased among patients treated for rejection (hazard ratio, 2.8; 95% confidence interval [CI], 1.2 to 6.6; P=0.02) and those receiving antithymocyte globulin induction therapy (hazard ratio, 2.5; 95% CI, 1.1 to 5.6; P=0.03); living-donor transplants were protective (hazard ratio, 0.2; 95% CI, 0.04 to 0.8; P=0.02). A higher-than-expected rejection rate was observed, with 1-year and 3-year estimates of 31% (95% CI, 24 to 40) and 41% (95% CI, 32 to 52), respectively. HIV infection remained well controlled, with stable CD4+ T-cell counts and few HIV-associated complications.
In this cohort of carefully selected HIV-infected patients, both patient- and graft-survival rates were high at 1 and 3 years, with no increases in complications associated with HIV infection. The unexpectedly high rejection rates are of serious concern and indicate the need for better immunotherapy. (Funded by the National Institute of Allergy and Infectious Diseases; ClinicalTrials.gov number, NCT00074386.).
感染人类免疫缺陷病毒(HIV)的患者接受肾移植和免疫抑制治疗的结果尚不完全清楚。
我们进行了一项前瞻性、非随机试验,纳入了接受肾移植的 HIV 感染候选者,这些候选者在接受稳定的抗逆转录病毒治疗方案时,其 CD4+T 细胞计数至少为 200 个/立方毫米,血浆 HIV 1 型(HIV-1)RNA 水平无法检测到。移植后的管理是根据研究方案进行的,这些方案定义了预防机会性感染的方法、活检指征以及可接受的免疫抑制、排斥反应管理和抗逆转录病毒治疗方法。
2003 年 11 月至 2009 年 6 月期间,共有 150 名患者接受了肾移植;幸存者的中位随访时间为 1.7 年。1 年和 3 年时患者生存率(±SD)分别为 94.6±2.0%和 88.2±3.8%,相应的平均移植物生存率分别为 90.4%和 73.7%。总的来说,这些生存率在国家数据库中报道的老年肾移植受者(≥65 岁)和所有肾移植受者的报道之间。多变量比例风险分析显示,接受排斥反应治疗(风险比,2.8;95%置信区间 [CI],1.2 至 6.6;P=0.02)和接受抗胸腺细胞球蛋白诱导治疗(风险比,2.5;95%CI,1.1 至 5.6;P=0.03)的患者发生移植物丢失的风险增加;活体供者移植具有保护作用(风险比,0.2;95%CI,0.04 至 0.8;P=0.02)。观察到排斥反应发生率高于预期,1 年和 3 年的估计值分别为 31%(95%CI,24 至 40)和 41%(95%CI,32 至 52)。HIV 感染得到了很好的控制,CD4+T 细胞计数稳定,HIV 相关并发症较少。
在本研究中,对精心挑选的 HIV 感染患者进行了队列研究,在 1 年和 3 年时患者和移植物的生存率均较高,没有增加与 HIV 感染相关的并发症。出乎意料的高排斥反应率令人严重关切,表明需要更好的免疫治疗。(由国家过敏和传染病研究所资助;临床试验.gov 编号,NCT00074386)。