Department of Occupational and Environmental Medicine, Lund University, Sweden.
BMC Public Health. 2010 Nov 22;10:716. doi: 10.1186/1471-2458-10-716.
Most epidemiologic studies use traffic at residential address as a surrogate for total traffic exposure when investigating effects of traffic on respiratory health. This study used GIS (Geographical Information Systems) to estimate traffic exposure, not only on residential, but also on workplace address, in addition to survey questions on time spent in traffic during commuting or other daily activities.The aim was to investigate 1) if there is an association between traffic exposure and prevalence of adult asthma and asthma symptoms, and 2) if so, does this association become stronger using more complete traffic exposure information.
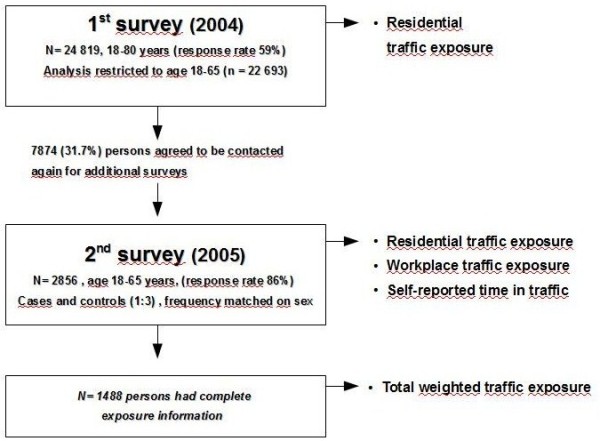
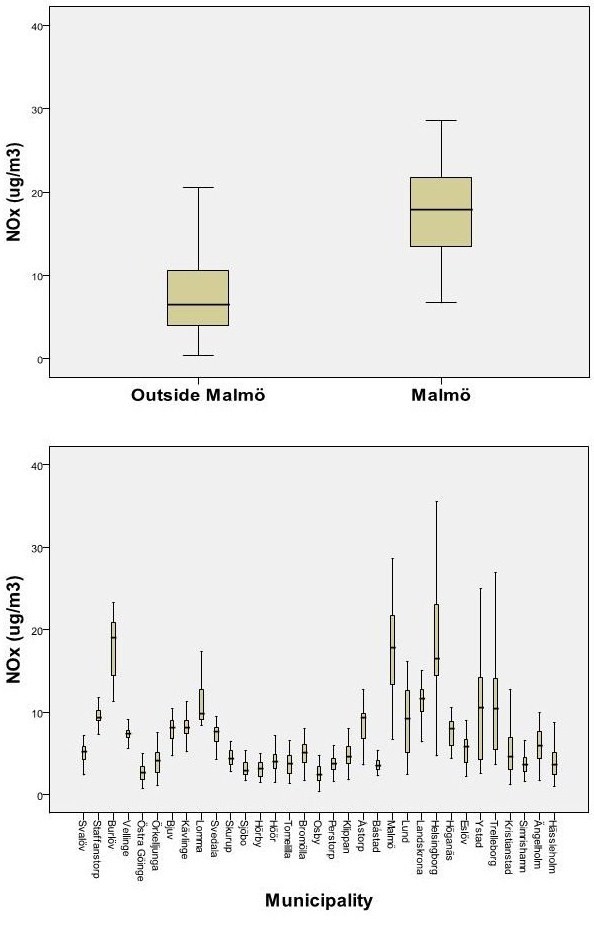
This study was conducted in two stages: A first cross-sectional survey in Southern Sweden 2004 (n = 24819, 18-80 years, response rate 59%) was followed by a case-control study in 2005 to obtain more detailed exposure and confounder information (n = 2856, asthmatics and controls (1:3), 86% response rate). In the first survey, only residential address was known. In the second survey, questions about workplace addresses and daily time spent in traffic were also included. Residential and workplace addresses were geocoded and linked with GIS to road data and dispersion modelled outdoor concentrations of NOx (annual mean, 250 × 250 m resolution).
Living within 50 m of a road (measured by GIS) with traffic intensity of >10 cars/minute (compared with no road within this distance) was associated with an increased prevalence of asthma, (OR = 1.8, 95% CI = (1.1-2.8), and with asthma symptoms last 12 months. No statistically significant effects were seen for traffic exposure at workplace address, daily time spent in traffic, or commuting time to work, after adjustment for confounders. A combined total exposure estimate did not give a stronger association with asthma prevalence or asthma symptoms.
Traffic exposure at close proximity to residential address showed association with asthma prevalence and asthma symptoms last 12 months, among adults in southern Sweden. The associations were not stronger when accounting for total traffic exposure. This could reflect exposure misclassfication at workplace address and for other daily time in traffic, but also that residential address remains the main determinant for traffic exposure among adults.
大多数流行病学研究使用居住地址的交通情况作为调查交通对呼吸道健康影响的总交通暴露的替代指标。本研究使用 GIS(地理信息系统)来估计交通暴露情况,不仅包括居住地址,还包括工作场所地址,此外还询问了通勤或其他日常活动中在交通中的时间。目的是调查 1)交通暴露与成人哮喘和哮喘症状的患病率之间是否存在关联,以及 2)如果存在关联,使用更完整的交通暴露信息是否会使这种关联变得更强。
本研究分两个阶段进行:2004 年在瑞典南部进行了一项横断面调查(n=24819,年龄 18-80 岁,应答率 59%),随后在 2005 年进行了病例对照研究,以获得更详细的暴露和混杂因素信息(n=2856,哮喘患者和对照者(1:3),应答率 86%)。在第一次调查中,只知道居住地址。在第二次调查中,还包括了工作场所地址和每日在交通中的时间。将居住和工作场所地址进行地理编码,并与 GIS 连接,以获取道路数据和扩散模型模拟的 NOx 场外浓度(年平均值,250×250m 分辨率)。
居住在距离道路 50m 以内(通过 GIS 测量),交通强度>10 辆/分钟(与距离道路 50m 以内没有道路相比),与哮喘的患病率增加有关(OR=1.8,95%CI=(1.1-2.8)),与过去 12 个月的哮喘症状有关。在校正混杂因素后,工作场所地址的交通暴露、每日在交通中的时间或通勤时间到工作场所,与哮喘患病率或哮喘症状之间没有统计学意义上的关联。总的交通暴露估计值并没有与哮喘患病率或哮喘症状之间的关联更强。
在瑞典南部,成年人居住地址附近的交通暴露与哮喘的患病率和过去 12 个月的哮喘症状有关。当考虑到总交通暴露时,这些关联并没有更强。这可能反映了工作场所地址和其他日常时间的交通暴露的暴露错误分类,但也反映了居住地址仍然是成年人交通暴露的主要决定因素。