Institute for Evaluative Research in Medicine, University of Bern, Stauffacherstrasse 78, CH-3014, Bern, Switzerland.
BMC Health Serv Res. 2010 Nov 23;10:315. doi: 10.1186/1472-6963-10-315.
Swiss ambulatory care is characterized by independent, and primarily practice-based, physicians, receiving fee for service reimbursement. This study analyses supply sensitive services using ambulatory care claims data from mandatory health insurance. A first research question was aimed at the hypothesis that physicians with large patient lists decrease their intensity of services and bill less per patient to health insurance, and vice versa: physicians with smaller patient lists compensate for the lack of patients with additional visits and services. A second research question relates to the fact that several cantons are allowing physicians to directly dispense drugs to patients ('self-dispensation') whereas other cantons restrict such direct sales to emergencies only. This second question was based on the assumption that patterns of rescheduling patients for consultations may differ across channels of dispensing prescription drugs and therefore the hypothesis of different consultation costs in this context was investigated.
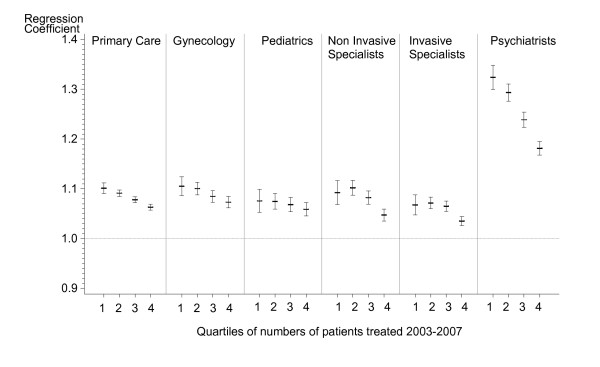
Complete claims data paid for by mandatory health insurance of all Swiss physicians in own practices were analyzed for the years 2003-2007. Medical specialties were pooled into six main provider types in ambulatory care: primary care, pediatrics, gynecology & obstetrics, psychiatrists, invasive and non-invasive specialists. For each provider type, regression models at the physician level were used to analyze the relationship between the number of patients treated and the total sum of treatment cost reimbursed by mandatory health insurance.
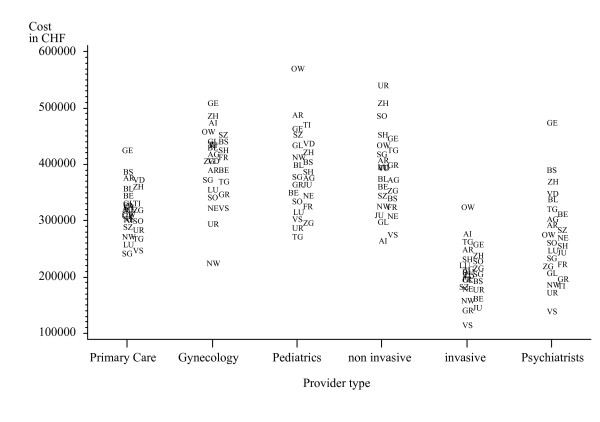
The results show non-proportional relationships between patient numbers and total sum of treatment cost for all provider types involved implying that treatment costs per patient increase with higher practice size. The related additional costs to the health system are substantial. Regions with self-dispensation had lowest treatment cost for primary care, gynecology, pediatrics and for psychiatrists whereas "prescription only" areas had lowest cost for specialists with non-invasive and invasive activities.
The results indicate that payment methods for services and for prescription drugs are associated with variations in treatment cost that are unlikely warranted by different medical needs of patients alone. Promoting physician accountability of care by linking reimbursements to quality, not quantity, of services are important policy measures to be considered for health care in Switzerland.
瑞士的门诊医疗服务以独立、主要基于实践的医生为特色,他们按服务收费。本研究使用强制性医疗保险的门诊医疗索赔数据来分析供应敏感服务。第一个研究问题旨在验证以下假设:患者人数多的医生会降低服务强度并减少每位患者的保险报销费用,反之亦然:患者人数少的医生会通过增加就诊次数和服务来弥补患者的不足。第二个研究问题涉及到这样一个事实,即几个州允许医生直接向患者发放药物(“自行配药”),而其他州则仅将此类直接销售限于紧急情况。这第二个问题基于这样一种假设,即通过不同渠道配药可能会改变患者重新预约就诊的模式,因此研究了这种情况下不同咨询费用的假设。
对 2003-2007 年所有在自己诊所执业的瑞士医生的强制性医疗保险支付的完整索赔数据进行了分析。将医疗专业合并为门诊医疗中的六种主要提供者类型:初级保健、儿科、妇产科、精神科、侵入性和非侵入性专家。对于每种提供者类型,使用医生层面的回归模型来分析治疗患者人数与强制性医疗保险报销的总治疗费用之间的关系。
结果表明,所有涉及的提供者类型的患者人数与总治疗费用之间存在非比例关系,这意味着每位患者的治疗费用随着实践规模的增加而增加。这对卫生系统相关的额外成本是巨大的。实行自行配药的地区,初级保健、妇产科、儿科和精神科的治疗费用最低,而“仅限处方”地区的非侵入性和侵入性活动专家的治疗费用最低。
结果表明,服务和处方药的支付方式与治疗费用的变化相关,而这些变化不太可能仅由患者不同的医疗需求来解释。通过将报销与服务质量而不是数量挂钩来促进医生对医疗保健的责任,是瑞士医疗保健需要考虑的重要政策措施。