Department of Anesthesiology, Institute of Clinical Medicine, University of Tromsø, N-9037 Tromsø, Norway.
Crit Care. 2010;14(6):R211. doi: 10.1186/cc9334. Epub 2010 Nov 23.
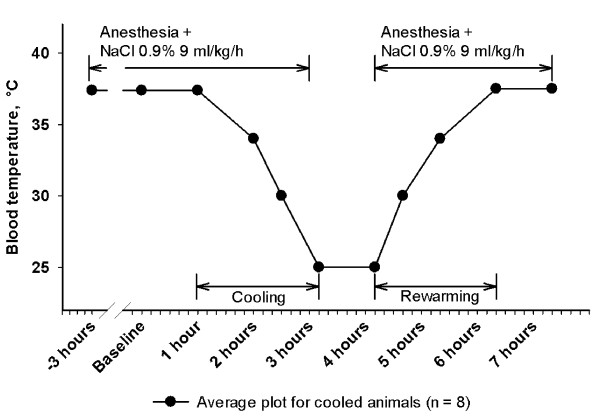
We developed a minimally invasive, closed chest pig model with the main aim to describe hemodynamic function during surface cooling, steady state severe hypothermia (one hour at 25°C) and surface rewarming.
Twelve anesthetized juvenile pigs were acutely catheterized for measurement of left ventricular (LV) pressure-volume loops (conductance catheter), cardiac output (Swan-Ganz), and for vena cava inferior occlusion. Eight animals were surface cooled to 25°C, while four animals were kept as normothermic time-matched controls.
During progressive cooling and steady state severe hypothermia (25°C) cardiac output (CO), stroke volume (SV), mean arterial pressure (MAP), maximal deceleration of pressure in the cardiac cycle (dP/dt(min)), indexes of LV contractility (preload recruitable stroke work, PRSW, and maximal acceleration of pressure in the cardiac cycle, dP/dt(max)) and LV end diastolic and systolic volumes (EDV and ESV) were significantly reduced. Systemic vascular resistance (SVR), isovolumetric relaxation time (Tau), and oxygen content in arterial and mixed venous blood increased significantly. LV end diastolic pressure (EDP) remained constant. After rewarming all the above mentioned hemodynamic variables that were depressed during 25°C remained reduced, except for CO that returned to pre-hypothermic values due to an increase in heart rate. Likewise, SVR and EDP were significantly reduced after rewarming, while Tau, EDV, ESV and blood oxygen content normalized. Serum levels of cardiac troponin T (TnT) and tumor necrosis factor-alpha (TNF-α) were significantly increased.
Progressive cooling to 25°C followed by rewarming resulted in a reduced systolic, but not diastolic left ventricular function. The post-hypothermic increase in heart rate and the reduced systemic vascular resistance are interpreted as adaptive measures by the organism to compensate for a hypothermia-induced mild left ventricular cardiac failure. A post-hypothermic increase in TnT indicates that hypothermia/rewarming may cause degradation of cardiac tissue. There were no signs of inadequate global oxygenation throughout the experiments.
我们开发了一种微创、闭胸猪模型,主要目的是描述表面冷却、稳定的重度低体温(1 小时 25°C)和表面复温期间的血液动力学功能。
12 只麻醉的幼年猪被急性置管以测量左心室(LV)压力-容积环(电导导管)、心输出量(Swan-Ganz)和下腔静脉闭塞。8 只动物进行表面冷却至 25°C,而 4 只动物作为正常体温的时间匹配对照。
在逐渐冷却和稳定的重度低体温(25°C)期间,心输出量(CO)、每搏量(SV)、平均动脉压(MAP)、心动周期中压力的最大减速(dP/dt(min))、LV 收缩性指数(预负荷可获得的每搏功,PRSW 和心动周期中压力的最大加速度,dP/dt(max))和 LV 舒张末期和收缩末期容积(EDV 和 ESV)显著降低。全身血管阻力(SVR)、等容舒张时间(Tau)和动脉及混合静脉血中的氧含量显著增加。LV 舒张末期压力(EDP)保持不变。复温后,除 CO 因心率增加而恢复到低体温前水平外,上述在 25°C 期间降低的所有血液动力学变量仍保持降低。同样,复温后 SVR 和 EDP 显著降低,而 Tau、EDV、ESV 和血液氧含量正常化。血清心肌肌钙蛋白 T(TnT)和肿瘤坏死因子-α(TNF-α)水平显著升高。
逐渐冷却至 25°C 后再复温导致收缩期而不是舒张期左心室功能降低。低体温后心率增加和全身血管阻力降低被解释为机体的适应性措施,以补偿低体温引起的轻度左心室心功能衰竭。低体温/复温后 TnT 升高表明可能导致心肌组织降解。整个实验过程中没有出现氧合不足的迹象。