Filseth Ole Magnus, Hermansen Stig Eggen, Kondratiev Timofei, Sieck Gary C, Tveita Torkjel
Anesthesia and Critical Care Research Group, Faculty of Health Sciences, Department of Clinical Medicine, UiT The Arctic University of Norway, Tromsø, Norway.
Division of Surgical Medicine and Intensive Care, University Hospital of North Norway, Tromsø, Norway.
Front Physiol. 2022 Mar 31;13:862729. doi: 10.3389/fphys.2022.862729. eCollection 2022.
Cooling by cardiopulmonary bypass (CPB) to deep hypothermic cardiac arrest (HCA) for cardiac surgical interventions, followed by CPB-rewarming is performed on a routine basis with relatively low mortality. In contrast, victims of deep accidental hypothermia rewarmed with CPB generally have a much worse prognosis. Thus, we have developed an intact pig model to compare effects on perfusion pressures and global oxygen delivery (DO) during immersion cooling versus cooling by CPB. Further, we compared the effects of CPB-rewarming between groups, to restitute cardiovascular function, brain blood flow, and brain metabolism.
Total sixteen healthy, anesthetized juvenile (2-3 months) castrated male pigs were randomized in a prospective, open placebo-controlled experimental study to immersion cooling (IMM , = 8), or cooling by CPB (CPB , = 8). After 75 minutes of deep HCA in both groups, pigs were rewarmed by CPB. After weaning from CPB surviving animals were observed for 2 h before euthanasia.
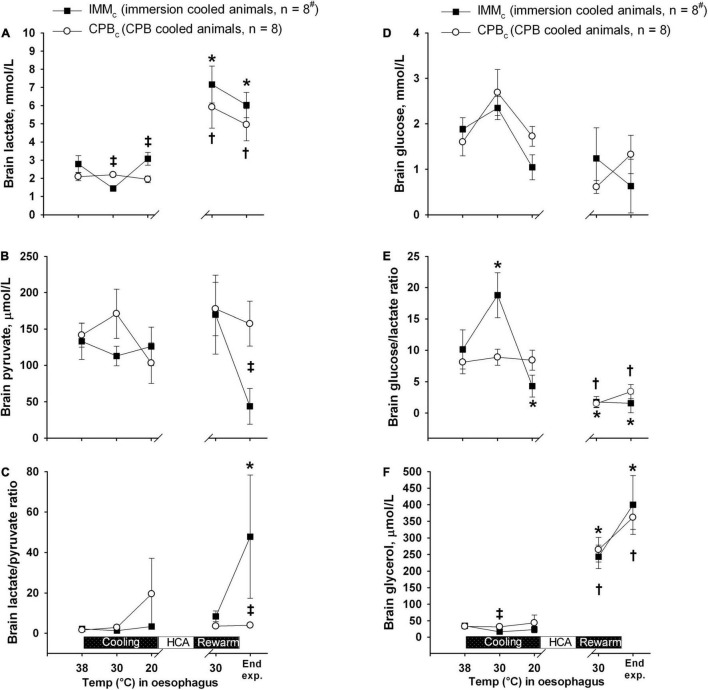
Survival rates at 2 h after completed rewarming were 4 out of 8 in the IMM group, and 8 out of 8 in the CPB group. Compared with the CPB -group, IMM animals showed significant reduction in DO, mean arterial pressure (MAP), cerebral perfusion pressure, and blood flow during cooling below 25°C as well as after weaning from CPB after rewarming. After rewarming, brain blood flow returned to control in CPB animals only, and brain micro dialysate-data showed a significantly increase in the lactate/pyruvate ratio in IMM vs. CPB animals.
Our data indicate that, although global O consumption was independent of DO, regional ischemic damage may have taken place during cooling in the brain of IMM animals below 25°C. The need for prolonged extracorporeal membrane oxygenation (ECMO) should be considered in all victims of accidental hypothermic arrest that cannot be weaned from CPB immediately after rewarming.
在心脏外科手术中,通过体外循环(CPB)将体温降至深低温心脏停搏(HCA),随后进行CPB复温,这种操作常规进行,死亡率相对较低。相比之下,通过CPB复温的意外深度低温受害者的预后通常要差得多。因此,我们建立了一个完整的猪模型,以比较浸泡冷却与CPB冷却对灌注压力和全身氧输送(DO)的影响。此外,我们比较了各组之间CPB复温对恢复心血管功能、脑血流量和脑代谢的影响。
在一项前瞻性、开放、安慰剂对照实验研究中,将总共16只健康的、麻醉的幼年(2 - 3个月)去势雄性猪随机分为浸泡冷却组(IMM组,n = 8)或CPB冷却组(CPB组,n = 8)。两组均进行75分钟的深低温心脏停搏后,通过CPB复温。在脱离CPB后,对存活的动物进行2小时观察,然后实施安乐死。
复温完成后2小时,IMM组8只中有4只存活,CPB组8只全部存活。与CPB组相比,IMM组动物在体温降至25°C以下时以及复温后脱离CPB后,DO、平均动脉压(MAP)、脑灌注压和血流量均显著降低。复温后,仅CPB组动物的脑血流量恢复至对照水平,脑微透析数据显示,IMM组动物的乳酸/丙酮酸比值相对于CPB组动物显著升高。
我们的数据表明,尽管总体氧消耗与DO无关,但在IMM组动物体温低于25°C的冷却过程中,脑部可能发生了局部缺血损伤。对于所有复温后不能立即脱离CPB的意外低温心脏停搏受害者,应考虑延长体外膜肺氧合(ECMO)的使用时间。