Yale University School of Medicine, New Haven, CT, USA.
Am Heart J. 2010 Nov;160(5):943-950.e1-5. doi: 10.1016/j.ahj.2010.06.046.
The Centers for Medicare and Medicaid Services provides public reporting on the quality of hospital care for patients with acute myocardial infarction (AMI). The Centers for Medicare and Medicaid Services Core Measures allow discretion in excluding patients because of relative contraindications to aspirin, β-blockers, and angiotensin-converting enzyme inhibitors. We describe trends in the proportion of patients with AMI with contraindications that could lead to discretionary exclusion from public reporting.
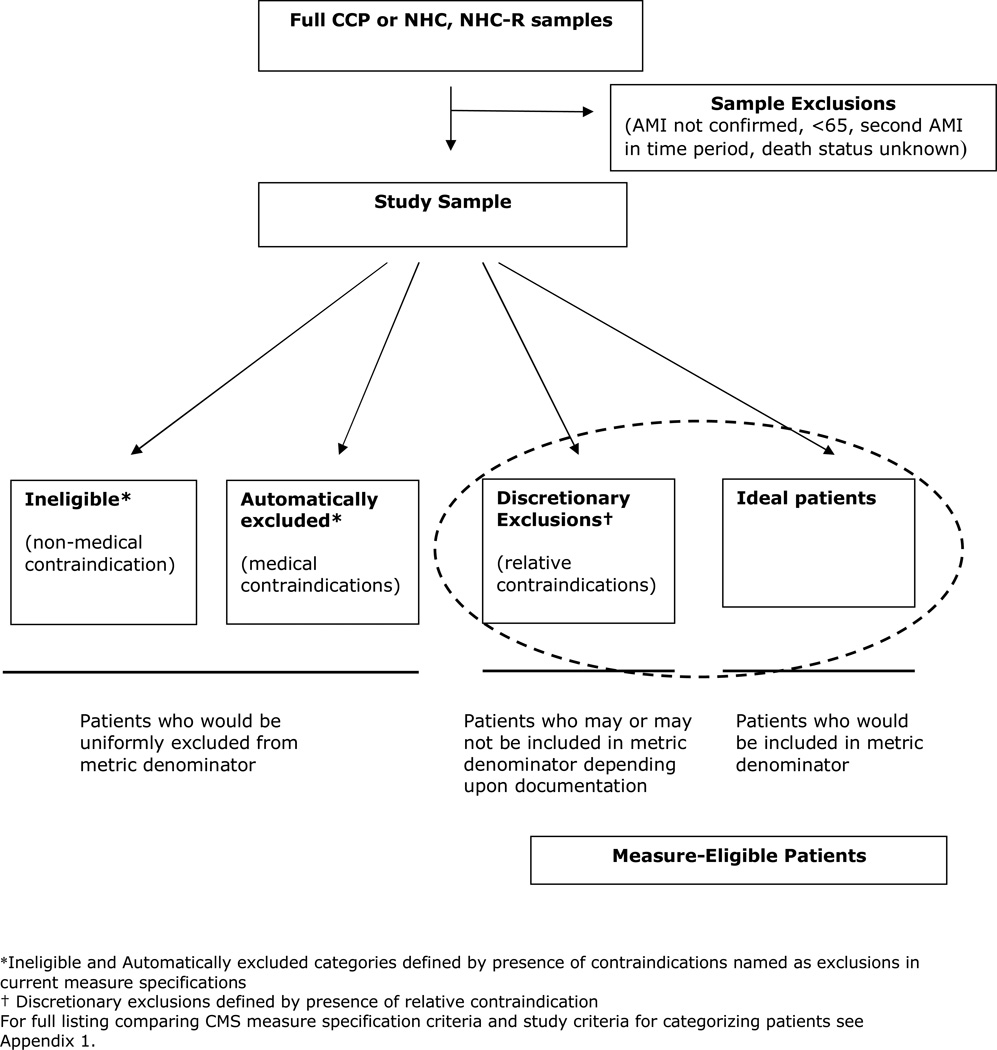
We completed cross-sectional analyses of 3 nationally representative data cohorts of AMI admissions among Medicare patients in 1994-1995 (n = 170,928), 1998-1999 (n = 27,432), and 2000-2001 (n = 27,300) from the national Medicare quality improvement projects. Patients were categorized as ineligible (eg, transfer patients), automatically excluded (specified absolute medical contraindications), discretionarily excluded (potentially excluded based on relative contraindications), or "ideal" for treatment for each measure.
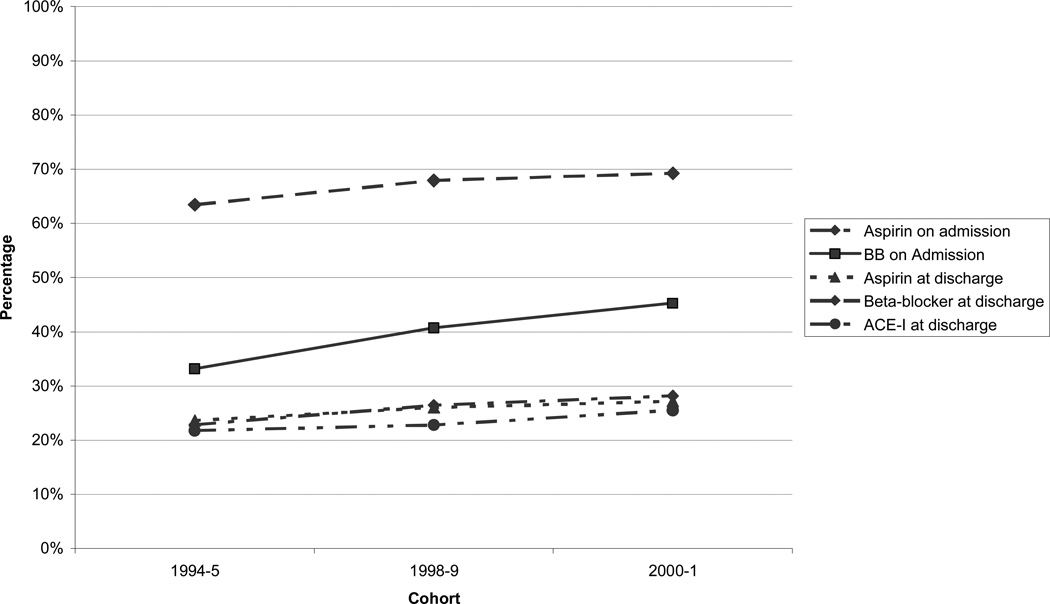
For 4 of 5 measures, the percentage of discretionarily excluded patients increased over the 3 periods (admission aspirin 15.8% to 16.9%, admission β-blocker 14.3% to 18.3%, discharge aspirin 10.3% to 12.3%, and angiotensin-converting enzyme inhibitors 2.8% to 3.9%; P < .001). Of patients potentially included in measures (those who were not ineligible or automatically excluded), the discretionarily excluded represented 25.5% to 69.2% in 2000-2001. Treatment rates among patients with discretionary exclusions also increased for 4 of 5 measures (all except angiotensin-converting enzyme inhibitors).
A sizeable and growing proportion of patients with AMI have relative contraindications to treatments that may result in discretionary exclusion from publicly reported quality measures. These patients represent a large population for which there is insufficient evidence as to whether measure exclusion or inclusion and treatment represents best care.
医疗保险和医疗补助服务中心为急性心肌梗死(AMI)患者的医院护理质量提供公共报告。医疗保险和医疗补助服务中心核心措施允许根据相对禁忌症(如阿司匹林、β受体阻滞剂和血管紧张素转换酶抑制剂)对患者进行自由裁量排除。我们描述了 AMI 患者因相对禁忌症而被自由裁量排除在公共报告之外的比例趋势。
我们对医疗保险质量改进计划中的全国 1994-1995 年(n = 170928)、1998-1999 年(n = 27432)和 2000-2001 年(n = 27300)三个全国代表性 AMI 入院数据队列进行了横断面分析。患者被归类为不合格(例如,转院患者)、自动排除(指定绝对医学禁忌症)、自由裁量排除(可能基于相对禁忌症排除)或每一项措施的“理想”治疗。
在五项措施中的四项中,自由裁量排除的患者比例在三个时期内有所增加(入院时阿司匹林 15.8%至 16.9%,入院时β受体阻滞剂 14.3%至 18.3%,出院时阿司匹林 10.3%至 12.3%,血管紧张素转换酶抑制剂 2.8%至 3.9%;P <.001)。在潜在纳入措施的患者中(即不合格或自动排除的患者),2000-2001 年自由裁量排除的患者占 25.5%至 69.2%。四项措施中的四项措施(除血管紧张素转换酶抑制剂外),自由裁量排除患者的治疗率也有所增加。
相当大比例且不断增长的 AMI 患者存在相对禁忌症,这些禁忌症可能导致其从公开报告的质量措施中被自由裁量排除。这些患者代表了一个很大的人群,对于他们是否排除或纳入措施以及治疗是否代表最佳护理,证据不足。