Barbash Ian J, Zhang Hongwei, Angus Derek C, Reis Steven E, Chang Chung-Chou H, Pike Francis R, Kahn Jeremy M
*Division of Pulmonary, Allergy, and Critical Care Medicine †Department of Critical Care Medicine, CRISMA Center, University of Pittsburgh School of Medicine ‡Department of Health Policy & Management, University of Pittsburgh Graduate School of Public Health §Clinical and Translational Science Institute, University of Pittsburgh ∥Division of Cardiology, University of Pittsburgh School of Medicine, Pittsburgh, PA.
Med Care. 2017 May;55(5):476-482. doi: 10.1097/MLR.0000000000000691.
One in 5 patients with acute myocardial infarction (AMI) are transferred between hospitals. However, current hospital performance measures based on AMI mortality exclude these patients from the evaluation of referral hospitals.
To determine the relationship between risk-standardized mortality for transferred and nontransferred patients at referral hospitals.
This is a retrospective cohort study.
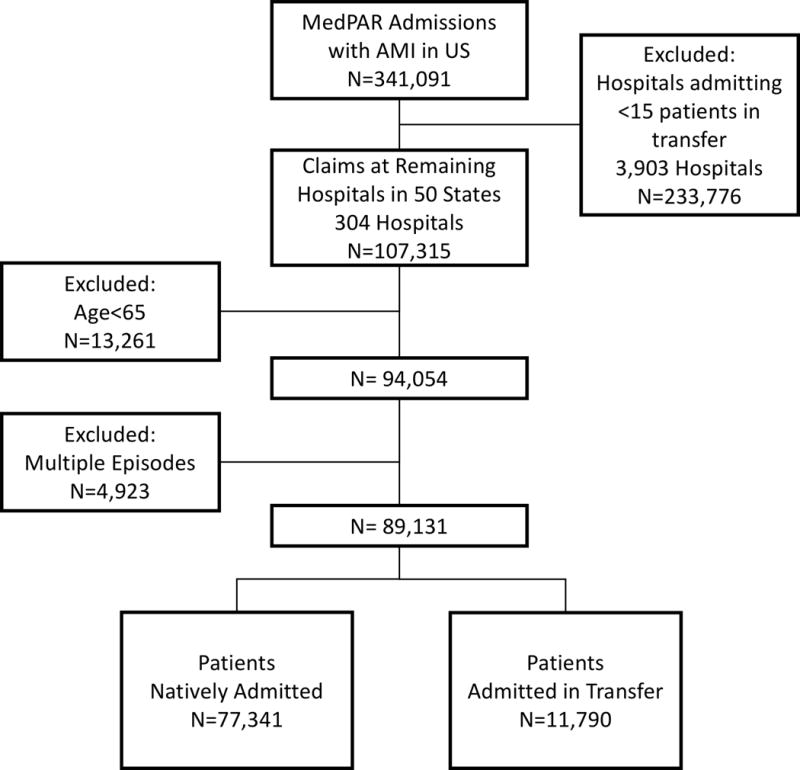
Fee-for-service Medicare claims from 2011 for patients hospitalized with a primary diagnosis of AMI, at hospitals admitting at least 15 patients in transfer.
Hospital-specific risk-standardized 30-day mortality rates (RSMRs) for 2 groups of patients: those admitted through transfer from another hospital, and those natively admitted without a preceding or subsequent interhospital transfer.
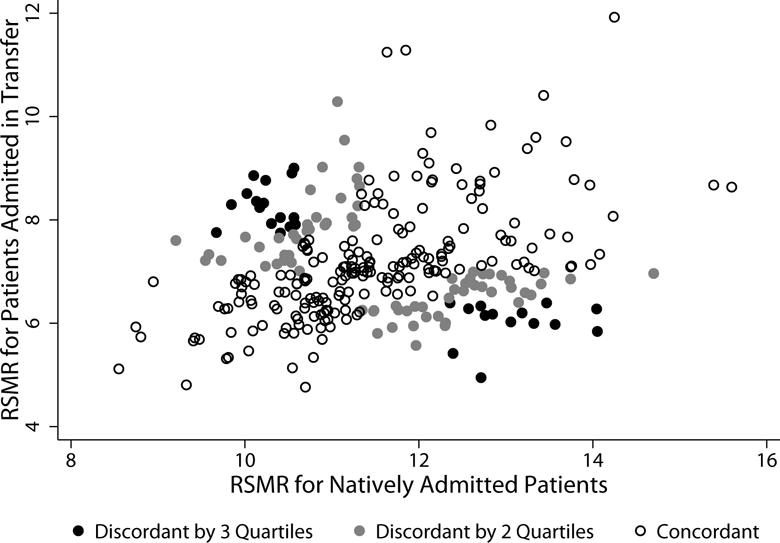
There were 304 hospitals admitting at least 15 patients in transfer. These hospitals cared for 77,711 natively admitted patients (median, 254; interquartile range, 162-321), and 11,829 patients admitted in transfer (median, 26; interquartile range, 19-46). Risk-standardized mortality rates were higher for natively admitted patients than for those admitted in transfer (mean, 11.5%±1.2% vs. 7.2%±1.1%). There was weak correlation between hospital performance as assessed by RSMR for patients natively admitted versus those admitted in transfer (Pearson r=0.24, P<0.001); when performance was arrayed by quartile, 102 hospitals (33.6%) differed at least 2 quartiles of performance across the 2 patient groups.
For Medicare patients with AMI, hospital-specific RSMRs for natively admitted patients are only weakly associated with RSMRs for patients transferred in from another hospital. Current AMI performance metrics may fail to provide guidance about hospital quality for transferred patients.
五分之一的急性心肌梗死(AMI)患者会在不同医院之间转诊。然而,目前基于AMI死亡率的医院绩效评估指标将这些患者排除在转诊医院的评估之外。
确定转诊医院中转诊患者和未转诊患者的风险标准化死亡率之间的关系。
这是一项回顾性队列研究。
2011年按服务收费的医疗保险索赔数据,涉及以AMI为主要诊断住院的患者,这些患者所在医院至少接收15例转诊患者。
两组患者的医院特定风险标准化30天死亡率(RSMRs):一组是从另一家医院转诊入院的患者,另一组是未经过院际转诊直接入院的患者。
有304家医院至少接收15例转诊患者。这些医院收治了77711例直接入院患者(中位数为254例;四分位间距为162 - 321例),以及11829例转诊入院患者(中位数为26例;四分位间距为19 - 46例)。直接入院患者的风险标准化死亡率高于转诊入院患者(平均分别为11.5%±1.2%和7.2%±1.1%)。对于直接入院患者和转诊入院患者,用RSMR评估的医院绩效之间存在弱相关性(Pearson相关系数r = 0.24,P < 0.001);当按四分位数排列绩效时,102家医院(33.6%)在两组患者中的绩效至少相差2个四分位数。
对于患有AMI的医疗保险患者,医院特定的直接入院患者RSMRs与从另一家医院转诊入院患者的RSMRs仅存在弱关联。当前的AMI绩效指标可能无法为转诊患者的医院质量提供指导。