Servei de Microbiologia, Hospital Universitari Germans Trias i Pujol, Fundació Institut en Ciències de Salut Germans Trias i Pujol, Badalona, Spain.
BMC Infect Dis. 2010 Dec 10;10:348. doi: 10.1186/1471-2334-10-348.
Individuals infected with human immunodeficiency virus (HIV) have an increased risk of progression to active tuberculosis following Mycobacterium tuberculosis infection. The objective of the study was to determine IFN-γ responses for the detection of latent tuberculosis infection (LTBI) with QuantiFERON-TB GOLD In Tube (QFT-G-IT) and T-SPOT.TB in HIV patients, and evaluate the influence of CD4 cell count on tests performance.
We studied 75 HIV patients enrolled for ongoing studies of LTBI with T-SPOT.TB, QFN-G-IT and TST. Mean CD4 cell counts ± standard deviation was 461.29 ± 307.49 cells/μl. Eight patients had a BCG scar.
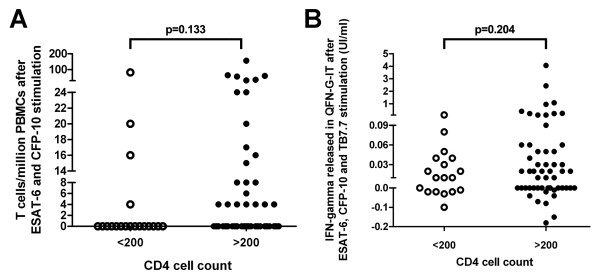
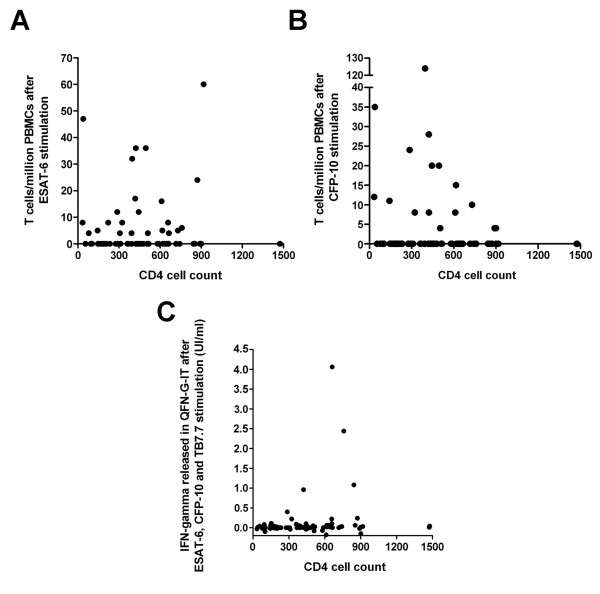
T-SPOT.TB, QFN-G-IT and TST were positive in 7 (9.3%), 5 (6.7%) and 9 (12%) cases, respectively. Global agreement between QFN-G-IT and T-SPOT.TB was 89% (κ = 0.275). The overall agreement of T-SPOT.TB and QFN-G-IT with TST was 80.8% (κ = 0.019) and 89% (κ = 0.373), respectively. We have found negative IFN-γ assays results among 2 BCG-vaccinated HIV-infected individuals with a positive TST. In non BCG-vaccinated patients, QFN-G-IT and TST were positive in 5 cases (7.5%) and T-SPOT.TB in 7 (10.4%). In contrast, in BCG-vaccinated patients, only TST was positive in 4/8 (50%) of the cases. The differences obtained in the number of positive results between TST and both IFN-γ assays in BCG vaccinated patients were significant (95% CI 3-97%, p = 0.046), however, the confidence interval is very wide given the small number of patients. In patients with CD4< 200, we obtained only one (5%) positive result with T-SPOT.TB; however, QFN-G-IT and TST were negative in all cases. On the contrary, percentages of positive results in patients with CD4> 200 were 10.9% (6/55), 9.1% (5/55) and 16.4% (9/55) with T-SPOT.TB, QFN-G-IT and TST, respectively.
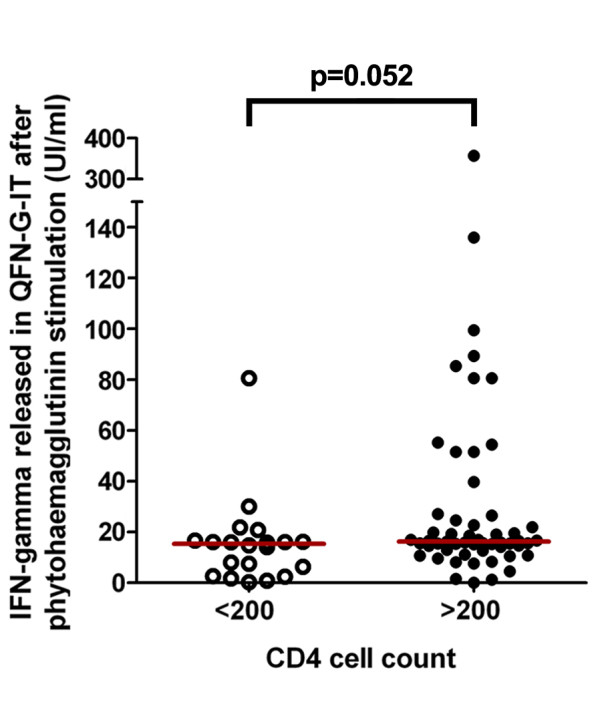
IFN-γ tests have the benefit over TST that are less influenced by BCG vaccination, consequently they are more specific than TST. Although our number of patients with advance immunosuppression is limited, our study suggests that IFN-γ assays are influenced with level of immunosuppression. The use of IFN-γ assays could be a helpful method for diagnosing LTBI in HIV population.
感染人类免疫缺陷病毒(HIV)的个体在感染结核分枝杆菌后进展为活动性肺结核的风险增加。本研究的目的是确定 IFN-γ 反应,以使用 QuantiFERON-TB GOLD In Tube(QFT-G-IT)和 T-SPOT.TB 检测潜伏性结核感染(LTBI),并评估 CD4 细胞计数对检测性能的影响。
我们研究了 75 名正在接受 T-SPOT.TB、QFN-G-IT 和 TST 检测 LTBI 的 HIV 患者。平均 CD4 细胞计数±标准偏差为 461.29±307.49 个/μl。8 例患者有卡介苗疤痕。
T-SPOT.TB、QFN-G-IT 和 TST 分别在 7(9.3%)、5(6.7%)和 9(12%)例中阳性。QFN-G-IT 和 T-SPOT.TB 之间的总体一致性为 89%(κ=0.275)。T-SPOT.TB 和 QFN-G-IT 与 TST 的总体一致性分别为 80.8%(κ=0.019)和 89%(κ=0.373)。我们发现 2 例 BCG 接种的 HIV 感染个体的 IFN-γ 检测结果为阴性,而 TST 为阳性。在未接种 BCG 的患者中,QFN-G-IT 和 TST 分别在 5 例(7.5%)和 T-SPOT.TB 在 7 例(10.4%)中阳性。相比之下,在 BCG 接种的患者中,只有 TST 在 4/8(50%)例中阳性。在 BCG 接种患者中,TST 和两种 IFN-γ 检测之间阳性结果的数量差异具有统计学意义(95%CI 3-97%,p=0.046),但由于患者数量较少,置信区间非常宽。在 CD4<200 的患者中,我们仅获得 T-SPOT.TB 阳性结果 1 例(5%);然而,所有情况下 QFN-G-IT 和 TST 均为阴性。相反,CD4>200 的患者中 T-SPOT.TB、QFN-G-IT 和 TST 的阳性结果百分比分别为 10.9%(6/55)、9.1%(5/55)和 16.4%(9/55)。
IFN-γ 检测比 TST 的优势在于其受卡介苗接种的影响较小,因此比 TST 更具特异性。尽管我们患有晚期免疫抑制的患者数量有限,但我们的研究表明 IFN-γ 检测受到免疫抑制水平的影响。IFN-γ 检测可作为 HIV 人群中诊断 LTBI 的有用方法。