Microbiology Service, Fundació Institut d'Investigació en Ciències de la Salut Germans Trias i Pujol, Hospital Universitari Germans Trias i Pujol, Universitat Autònoma de Barcelona, Badalona, Spain.
PLoS One. 2010 Nov 30;5(11):e14132. doi: 10.1371/journal.pone.0014132.
Current treatment of chronic hepatitis C virus (HCV) infection has limited efficacy -especially among genotype 1 infected patients-, is costly, and involves severe side effects. Thus, predicting non-response is of major interest for both patient wellbeing and health care expense. At present, treatment cannot be individualized on the basis of any baseline predictor of response. We aimed to identify pre-treatment clinical and virological parameters associated with treatment failure, as well as to assess whether therapy outcome could be predicted at baseline.
Forty-three HCV subtype 1b (HCV-1b) chronically infected patients treated with pegylated-interferon alpha plus ribavirin were retrospectively studied (21 responders and 22 non-responders). Host (gender, age, weight, transaminase levels, fibrosis stage, and source of infection) and viral-related factors (viral load, and genetic variability in the E1-E2 and Core regions) were assessed. Logistic regression and discriminant analyses were used to develop predictive models. A "leave-one-out" cross-validation method was used to assess the reliability of the discriminant models.
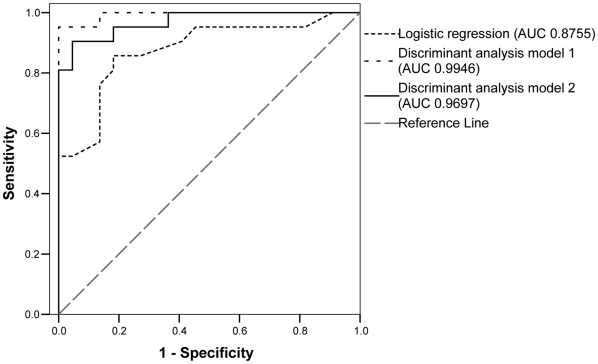
Lower alanine transaminase levels (ALT, p=0.009), a higher number of quasispecies variants in the E1-E2 region (number of haplotypes, nHap_E1-E2) (p=0.003), and the absence of both amino acid arginine at position 70 and leucine at position 91 in the Core region (p=0.039) were significantly associated with treatment failure. Therapy outcome was most accurately predicted by discriminant analysis (90.5% sensitivity and 95.5% specificity, 85.7% sensitivity and 81.8% specificity after cross-validation); the most significant variables included in the predictive model were the Core amino acid pattern, the nHap_E1-E2, and gamma-glutamyl transferase and ALT levels.
Discriminant analysis has been shown as a useful tool to predict treatment outcome using baseline HCV genetic variability and host characteristics. The discriminant models obtained in this study led to accurate predictions in our population of Spanish HCV-1b treatment naïve patients.
目前慢性丙型肝炎病毒(HCV)感染的治疗效果有限 - 尤其是在感染基因型 1 的患者中 - 且费用高昂,还伴有严重的副作用。因此,对于患者的健康和医疗费用而言,预测无应答具有重要意义。目前,无法根据任何治疗应答的基线预测因子来进行个体化治疗。我们旨在确定与治疗失败相关的治疗前临床和病毒学参数,并评估是否可以在基线时预测治疗结果。
我们回顾性研究了 43 例慢性 HCV-1b 感染患者(21 例应答者和 22 例无应答者)接受聚乙二醇干扰素 α 加利巴韦林治疗的情况。评估了宿主(性别、年龄、体重、转氨酶水平、纤维化分期和感染源)和病毒相关因素(病毒载量以及 E1-E2 和核心区的遗传变异性)。采用逻辑回归和判别分析建立预测模型。采用“逐一剔除”交叉验证方法评估判别模型的可靠性。
较低的丙氨酸转氨酶水平(ALT,p=0.009)、E1-E2 区更多的准种变异数(nHap_E1-E2)(p=0.003)以及核心区缺乏精氨酸 70 位和亮氨酸 91 位(p=0.039)与治疗失败显著相关。判别分析能最准确地预测治疗结果(90.5%的敏感性和 95.5%的特异性,交叉验证后的敏感性和特异性分别为 85.7%和 81.8%);纳入预测模型的最显著变量包括核心区氨基酸模式、nHap_E1-E2、γ-谷氨酰转移酶和 ALT 水平。
判别分析已被证明是一种有用的工具,可利用基线 HCV 遗传变异性和宿主特征预测治疗结果。本研究获得的判别模型在我们的西班牙 HCV-1b 初治患者人群中实现了准确的预测。