Department of Intensive Care, Erasme University Hospital, Université Libre de Bruxelles, Route de Lennik 808, 1070 Brussels, Belgium.
Intensive Care Med. 2011 Feb;37(2):233-40. doi: 10.1007/s00134-010-2098-8. Epub 2010 Dec 10.
Second-generation FloTrac software has been shown to reliably measure cardiac output (CO) in cardiac surgical patients. However, concerns have been raised regarding its accuracy in vasoplegic states. The aim of the present multicenter study was to investigate the accuracy of the third-generation software in patients with sepsis, particularly when total systemic vascular resistance (TSVR) is low.
Fifty-eight septic patients were included in this prospective observational study in four university-affiliated ICUs. Reference CO was measured by bolus pulmonary thermodilution (iCO) using 3-5 cold saline boluses. Simultaneously, CO was computed from the arterial pressure curve recorded on a computer using the second-generation (CO(G2)) and third-generation (CO(G3)) FloTrac software. CO was also measured by semi-continuous pulmonary thermodilution (CCO).
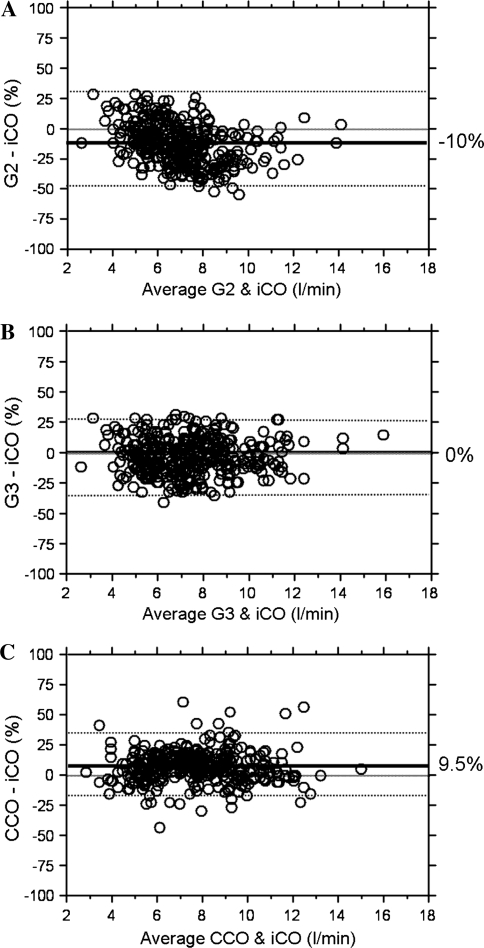
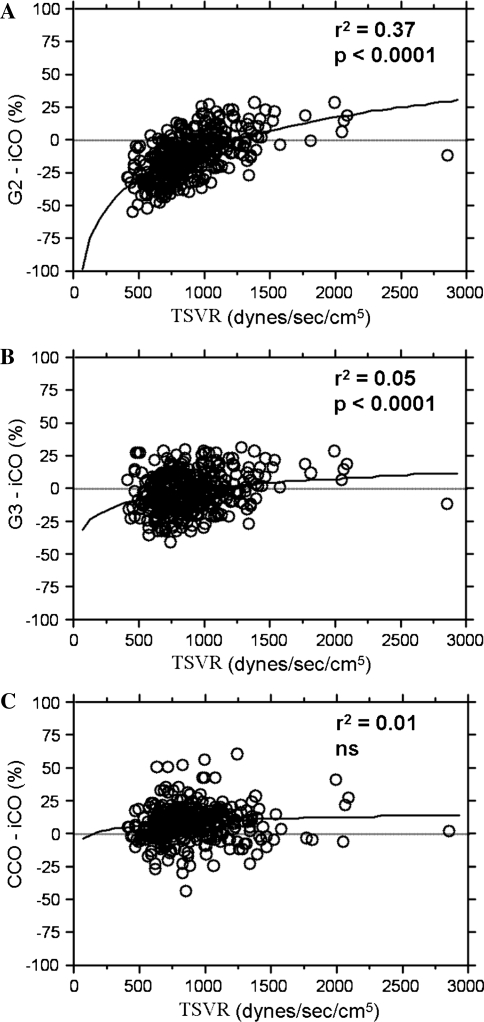
A total of 401 simultaneous measurements of iCO, CO(G2), CO(G3), and CCO were recorded. The mean (95%CI) biases between CO(G2) and iCO, CO(G3) and iCO, and CCO and iCO were -10 (-15 to -5)% [-0.8 (-1.1 to -0.4) L/min], 0 (-4 to 4)% [0 (-0.3 to 0.3) L/min], and 9 (6-13)% [0.7 (0.5-1.0) L/min], respectively. The percentage errors were 29 (20-37)% for CO(G2), 30 (24-37)% for CO(G3), and 28 (22-34)% for CCO. The difference between iCO and CO(G2) was significantly correlated with TSVR (r(2) = 0.37, p < 0.0001). A very weak (r(2) = 0.05) relationship was also observed for the difference between iCO and CO(G3).
In patients with sepsis, the third-generation FloTrac software is more accurate, as precise, and less influenced by TSVR than the second-generation software.
第二代 FloTrac 软件已被证明可在心脏外科患者中可靠地测量心输出量(CO)。然而,人们对其在血管扩张状态下的准确性提出了担忧。本多中心研究的目的是调查第三代软件在脓毒症患者中的准确性,特别是在总全身血管阻力(TSVR)较低时。
在四家大学附属医院的四个 ICU 中,对 58 例脓毒症患者进行了这项前瞻性观察性研究。参考 CO 通过肺动脉热稀释法(iCO)使用 3-5 个冷盐水弹丸测量。同时,使用第二代(CO(G2))和第三代(CO(G3))FloTrac 软件从计算机上记录的动脉压力曲线上计算 CO。CO 也通过半连续肺动脉热稀释法(CCO)测量。
共记录了 401 次 iCO、CO(G2)、CO(G3)和 CCO 的同步测量值。CO(G2)与 iCO、CO(G3)与 iCO 和 CCO 与 iCO 的平均(95%CI)偏差分别为-10(-15 至-5)%[-0.8(-1.1 至-0.4)L/min]、0(-4 至 4)%[0(-0.3 至 0.3)L/min]和 9(6-13)%[0.7(0.5-1.0)L/min]。CO(G2)的百分比误差为 29(20-37)%,CO(G3)的百分比误差为 30(24-37)%,CCO 的百分比误差为 28(22-34)%。iCO 和 CO(G2)之间的差值与 TSVR 显著相关(r(2)=0.37,p<0.0001)。iCO 和 CO(G3)之间的差值也存在较弱的相关性(r(2)=0.05)。
在脓毒症患者中,第三代 FloTrac 软件比第二代软件更准确、更精确,并且受 TSVR 的影响更小。