Department of Health Policy & Management, Bloomberg School of Public Health, Johns Hopkins University, 624 N, Broadway, Baltimore, MD 21205, USA.
BMC Health Serv Res. 2010 Dec 20;10:343. doi: 10.1186/1472-6963-10-343.
Predictive modeling presents an opportunity to contain the expansion of medical expenditures by focusing on very few people. Evaluation of how risk adjustment models perform in predictive modeling in Taiwan or Asia has been rare. The aims of this study were to evaluate the performance of different risk adjustment models (the ACG risk adjustment system and prior expenditures) in predictive modeling, using Taiwan's National Health Insurance (NHI) claims data, and to compare characteristics of potentially high-expenditure subjects identified through different models.
A random sample of NHI enrollees continuously enrolled in 2002 and 2003 (n = 164,562) was selected. Health status measures and total expenditures derived from 2002 NHI claims data were used to predict the possibility of becoming 2003 top users. Statistics-based indicators (C-statistics, sensitivity, & Predictive Positive Value) and characteristics of identified top groups by different models (expenditures and prevalence of manageable diseases) were presented.
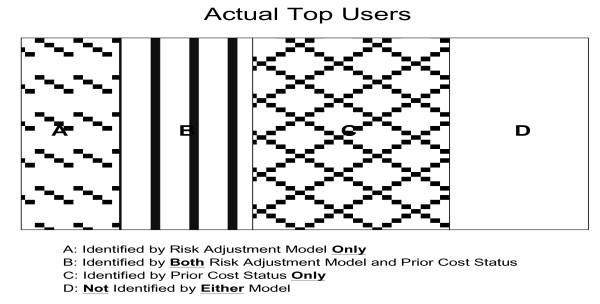
Both diagnosis-based and prior expenditures models performed much better than the demographic model. Diagnosis-based models were better in identifying top users with manageable diseases; prior expenditures models were better in statistics-based indicators and identifying people with higher average expenditures. Prior expenditures status could correctly identify more actual top users than diagnosis-based or demographic models. The proportions of actual top users that could be identified by diagnosis-based models alone were much lower than that identified by prior expenditures status.
Predicted top users identified by different models have different characteristics and there is little agreement between modes regarding which groups would be potentially top users; therefore, which model to use should depend on the purpose of predictive modeling. Prior expenditures are a more powerful tool than diagnosis-based risk adjusters in terms of correctly identifying more actual high expenditures users. There is still much room left for improvement of diagnosis-based models in predictive modeling.
预测建模为通过关注极少数人来控制医疗支出的扩张提供了机会。评估风险调整模型在台湾或亚洲的预测建模中的表现情况很少见。本研究的目的是使用台湾全民健康保险(NHI)理赔数据评估不同风险调整模型(ACG 风险调整系统和既往支出)在预测建模中的表现,并比较通过不同模型识别的高支出潜在人群的特征。
从 2002 年和 2003 年连续参保的 NHI 参保者中随机抽取样本(n = 164562)。使用 2002 年 NHI 理赔数据中的健康状况指标和总支出来预测成为 2003 年高支出者的可能性。呈现基于统计的指标(C 统计量、敏感性和预测阳性值)以及不同模型(可管理疾病的支出和患病率)识别的高支出组的特征。
基于诊断的模型和既往支出模型的表现均优于人口统计学模型。基于诊断的模型在识别有可管理疾病的高支出者方面更好;既往支出模型在基于统计的指标和识别高平均支出人群方面更好。既往支出状况可以比基于诊断或人口统计学的模型更准确地识别更多实际的高支出者。基于诊断的模型单独识别的实际高支出者的比例远低于既往支出状况识别的比例。
不同模型识别的预测高支出者具有不同的特征,不同模式之间对于哪些群体可能成为潜在高支出者的看法存在分歧;因此,应根据预测建模的目的选择使用哪种模型。从正确识别更多实际高支出用户的角度来看,既往支出比基于诊断的风险调整器更具优势。基于诊断的模型在预测建模方面仍有很大的改进空间。