Department of Internal Medicine, Harold C. Simmons Cancer Center, University of Texas Southwestern Medical Center, Dallas, Texas, USA.
J Thorac Oncol. 2011 Feb;6(2):365-71. doi: 10.1097/JTO.0b013e3181fff142.
: Recent clinical trials incorporating maintenance chemotherapy into the initial treatment of advanced non-small cell lung cancer (NSCLC) have highlighted the benefits of exposing patients to second-line therapies. We, therefore, determined the predictors and impact of second-line chemotherapy administration in a contemporary, diverse NSCLC population.
: We performed a retrospective analysis of consecutive patients diagnosed with stage IV NSCLC from 2000 to 2007 at clinical facilities associated with the University of Texas Southwestern Medical Center. Demographic, disease, treatment, and outcome data were obtained from hospital tumor registries. The association between these variables was assessed using univariate analysis and multivariate logistic regression.
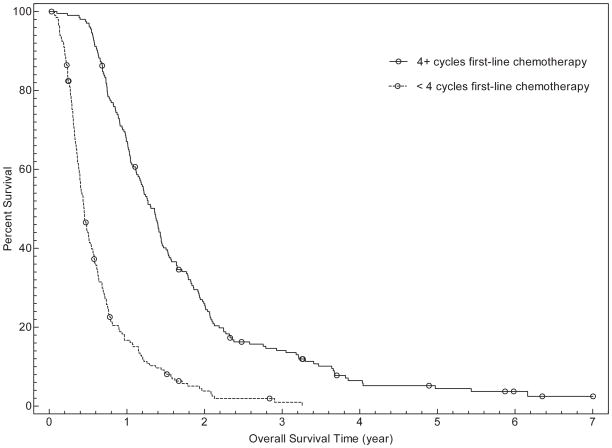
: A total of 406 patients in this cohort received first-line chemotherapy and were included in the analysis. Mean age was 59 years, 28% were women, and 59% were white. Among these patients, 197 (49%) received second-line chemotherapy. Among those patients who had not progressed after four to six cycles of first-line chemotherapy, 67% received second-line chemotherapy. Receipt of second-line chemotherapy was significantly associated with patient insurance type (p = 0.007), number of cycles of first-line chemotherapy (p < 0.001), and receipt of prechemotherapy palliative radiation therapy (p = 0.005) but was not associated with patient age, gender, race, histology, or year of diagnosis. In a multivariate model, second-line chemotherapy administration remained associated with insurance type (p = 0.003), number of cycles of first-line chemotherapy (p < 0.001), and receipt of prechemotherapy palliative radiation therapy (p = 0.008). The number of cycles of first-line chemotherapy and administration of second-line chemotherapy were associated with overall survival in both univariate and multivariate analyses.
: In this unselected, contemporary, and diverse cohort of patients with advanced NSCLC, 67% of individuals whose disease had not progressed after four to six cycles of first-line chemotherapy eventually received second-line chemotherapy. Markers of socioeconomic status, symptom burden, and response to and tolerance of first-line chemotherapy were associated with receipt of second-line chemotherapy. These factors may assist in the selection of patients most likely to benefit from maintenance chemotherapy.
最近的临床试验将维持化疗纳入晚期非小细胞肺癌(NSCLC)的初始治疗,突出了使患者接受二线治疗的益处。因此,我们在当代多样化的 NSCLC 人群中确定了接受二线化疗的预测因素和影响。
我们对 2000 年至 2007 年在德克萨斯大学西南医学中心附属医院就诊的连续 IV 期 NSCLC 患者进行了回顾性分析。从医院肿瘤登记处获得人口统计学、疾病、治疗和结局数据。使用单变量分析和多变量逻辑回归评估这些变量之间的关联。
该队列中有 406 例患者接受了一线化疗并纳入分析。平均年龄为 59 岁,28%为女性,59%为白人。在这些患者中,197 例(49%)接受了二线化疗。在一线化疗 4-6 个周期后未进展的患者中,有 67%接受了二线化疗。接受二线化疗与患者的保险类型显著相关(p=0.007),与一线化疗的周期数显著相关(p<0.001),与化疗前姑息性放疗显著相关(p=0.005),但与患者的年龄、性别、种族、组织学或诊断年份无关。在多变量模型中,二线化疗的应用仍与保险类型相关(p=0.003),与一线化疗的周期数相关(p<0.001),与化疗前姑息性放疗相关(p=0.008)。一线化疗的周期数和二线化疗的应用与单变量和多变量分析中的总生存相关。
在这个未选择的、当代的和多样化的晚期 NSCLC 患者队列中,在一线化疗 4-6 个周期后疾病未进展的患者中,有 67%最终接受了二线化疗。社会经济地位、症状负担以及对一线化疗的反应和耐受性的标志物与二线化疗的应用相关。这些因素可能有助于选择最有可能从维持化疗中获益的患者。