Banks Kamakki, Lo Monica, Khera Amit
From the Donald W. Reynolds Cardiovascular Clinical Research Center, the University of Texas Southwestern Medical Center, Dallas TX.
Curr Cardiol Rev. 2010 Feb;6(1):71-81. doi: 10.2174/157340310790231608.
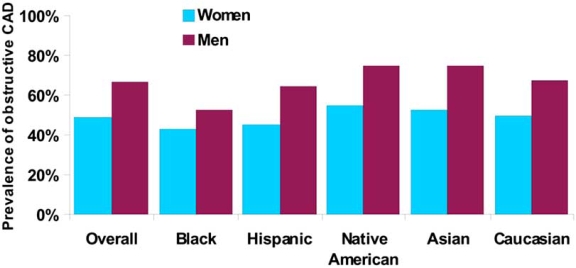
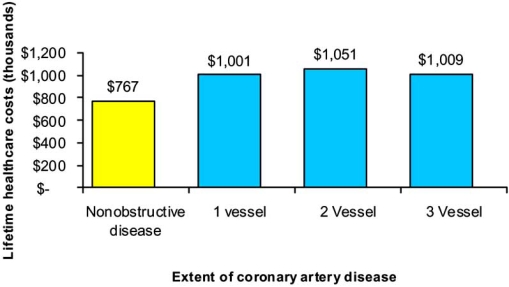
Angina in the absence of obstructive coronary artery disease, sometimes referred to as cardiac syndrome X (CSX), is a debilitating condition that disproportionately affects women. More than 50% of women evaluated for angina have non-obstructive disease by cardiac catheterization, although the total numbers of women affected by CSX are unknown. Varying clinical definitions and the lack of large scale epidemiologic studies focusing on this illness have resulted in limited knowledge about its risk factors, although there appears to be an association with black race, estrogen deficiency, and insulin resistance. Contrary to prior beliefs about the benign nature of this entity, these women suffer considerable morbidity with costly economic implications that approach the lifetime costs of healthcare utilization for those with obstructive coronary disease. Two prevailing hypotheses have emerged to explain CSX: the ischemic hypothesis detailing abnormal coronary microvascular function and the non-ischemic hypothesis describing altered pain perception and myocardial hypersensitivity. Treatment strategies have focused on both of these pathways with the main goal of improving symptoms. Beta blockers provide the most convincing evidence for benefit, with other antianginals having secondary roles. Other promising pharmacologic therapies include xanthine derivatives, estrogen replacement therapy, ACE inhibitors, and statin medications, among other emerging treatment options. Neurostimulation and lifestyle factors including exercise can also be beneficial in reducing symptoms. However, managing patients with CSX can be frustrating for both patients and physicians, as there is a lack of data regarding an optimal treatment algorithm including few large-scale randomized controlled trials to clarify effective therapies.
无阻塞性冠状动脉疾病的心绞痛,有时被称为心脏综合征X(CSX),是一种使人衰弱的病症,对女性的影响尤为严重。接受心绞痛评估的女性中,超过50%通过心脏导管检查显示为非阻塞性疾病,尽管受CSX影响的女性总数尚不清楚。由于临床定义各异,且缺乏针对该疾病的大规模流行病学研究,导致对其危险因素的了解有限,尽管似乎与黑人种族、雌激素缺乏和胰岛素抵抗有关。与之前认为该病症性质良性的观点相反,这些女性遭受相当大的发病率,带来高昂的经济影响,接近阻塞性冠状动脉疾病患者一生的医疗保健使用成本。出现了两种流行的假说来解释CSX:缺血假说详述了冠状动脉微血管功能异常,非缺血假说描述了疼痛感知改变和心肌超敏反应。治疗策略聚焦于这两条途径,主要目标是改善症状。β受体阻滞剂提供了最有说服力的获益证据,其他抗心绞痛药物起次要作用。其他有前景的药物治疗包括黄嘌呤衍生物、雌激素替代疗法、ACE抑制剂和他汀类药物,以及其他新兴治疗选择。神经刺激和包括运动在内的生活方式因素也有助于减轻症状。然而,管理CSX患者对患者和医生来说都可能令人沮丧,因为缺乏关于最佳治疗方案的数据,包括很少有大规模随机对照试验来阐明有效疗法。