Division of Infectious Diseases, Johns Hopkins School of Medicine, Baltimore Maryland, United States of America.
PLoS One. 2011 Jan 27;6(1):e15738. doi: 10.1371/journal.pone.0015738.
It remains controversial as to whether HIV-1 subtypes influence disease progression. Singapore offers a unique opportunity to address this issue due to the presence of co-circulating subtypes. We compared subtype CRF01_AE and non-CRF01_AE infected patients, with regards to estimated annual rate of CD4+ T-cell loss and time from estimated data of seroconversion (EDS) to antiretroviral therapy (ART).
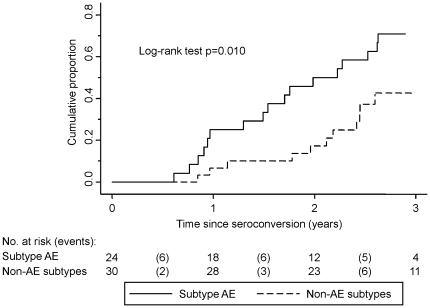
We recruited ART-naive patients with known dates of seroconversion between October 2002 and December 2007 at the Singapore Communicable Disease Centre, the national reference treatment centre. Multilevel mixed-effects models were used to analyse the rate of CD4+ T-cell decline. Time from EDS to ART was analyzed with the Kaplan-Meier survival method and compared with Cox proportional hazards models.
54 patients with previously assigned HIV-1 subtypes (24 CRF01_AE, 17 B, 8 B', 1 CRF33_01B, 3 CRF34_01B and 1 G) were observed for 89 patient-years. Subtype CRF01_AE and non-CRF01_AE infected patients did not differ in age, gender, risk factor, rate of symptomatic seroconversion, baseline CD4+ T-cell count, log(10) viral load or haemoglobin concentration. The estimated annual rate of CD4+ T-cell loss was 58 cells/mm(3)/year (95% CI: 7 to 109; P = 0.027) greater in subtype CRF01_AE infected patients compared to non-CRF01_AE patients, after adjusting for age, baseline CD4+ T-cell count and baseline log(10) viral load. The median time from EDS to ART was 1.8 years faster comparing CRF01_AE to non-CRF01_AE infected patient with a 2.5 times (95% CI: 1.2-5.0; P = 0.013) higher hazard for ART initiation, after controlling for age, baseline CD4+ T-cell count and baseline log(10) viral load.
Infecting subtype significantly impacted the rate of CD4+ T-cell loss and time to treatment in this cohort. Studies to understand the biological basis for this difference could further our understanding of HIV pathogenesis.
HIV-1 亚型是否会影响疾病进展仍存在争议。新加坡由于存在共循环的亚型,为解决这一问题提供了独特的机会。我们比较了感染 CRF01_AE 和非 CRF01_AE 的患者,评估了每年 CD4+T 细胞损失的估计速度以及从血清转换估计日期 (EDS) 到抗逆转录病毒治疗 (ART) 的时间。
我们招募了 2002 年 10 月至 2007 年 12 月在新加坡传染病中心(国家参考治疗中心)有已知血清转换日期的、接受 ART 治疗的初治患者。使用多水平混合效应模型分析 CD4+T 细胞下降率。用 Kaplan-Meier 生存法分析从 EDS 到 ART 的时间,并与 Cox 比例风险模型进行比较。
观察了 54 名以前分配有 HIV-1 亚型(24 名 CRF01_AE、17 名 B、8 名 B'、1 名 CRF33_01B、3 名 CRF34_01B 和 1 名 G)的患者 89 患者年。CRF01_AE 和非 CRF01_AE 感染患者在年龄、性别、危险因素、有症状血清转换率、基线 CD4+T 细胞计数、log10 病毒载量或血红蛋白浓度方面没有差异。在调整年龄、基线 CD4+T 细胞计数和基线 log10 病毒载量后,CRF01_AE 感染患者每年 CD4+T 细胞损失估计速度比非 CRF01_AE 患者高 58 个细胞/mm3/年(95%CI:7-109;P=0.027)。在调整年龄、基线 CD4+T 细胞计数和基线 log10 病毒载量后,CRF01_AE 感染患者从 EDS 到 ART 的中位时间比非 CRF01_AE 感染患者快 1.8 年,ART 启动的风险高 2.5 倍(95%CI:1.2-5.0;P=0.013)。
在本队列中,感染亚型显著影响 CD4+T 细胞损失速度和治疗时间。研究了解这种差异的生物学基础可以进一步加深我们对 HIV 发病机制的理解。