Gangcuangco Louie Mar A, Eustaquio Patrick C
Hawaii Center for AIDS, John A Burns School of Medicine, University of Hawaii at Manoa, Honolulu, HI 96813, USA.
Love Yourself, Inc., Mandaluyong 1552, Metro Manila, Philippines.
Trop Med Infect Dis. 2023 Apr 30;8(5):258. doi: 10.3390/tropicalmed8050258.
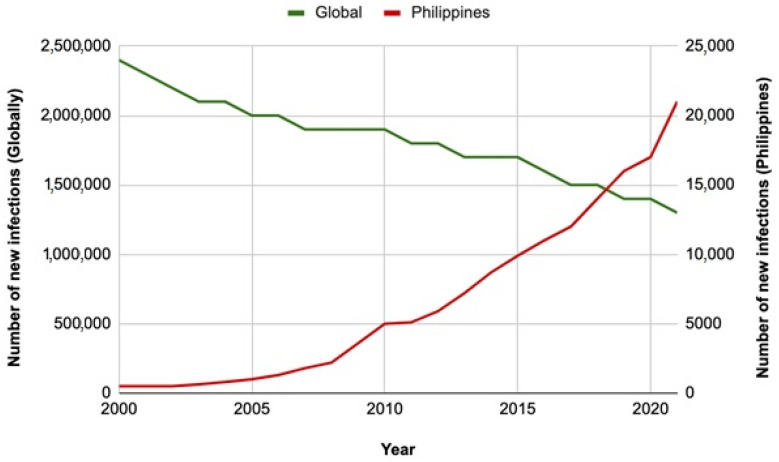
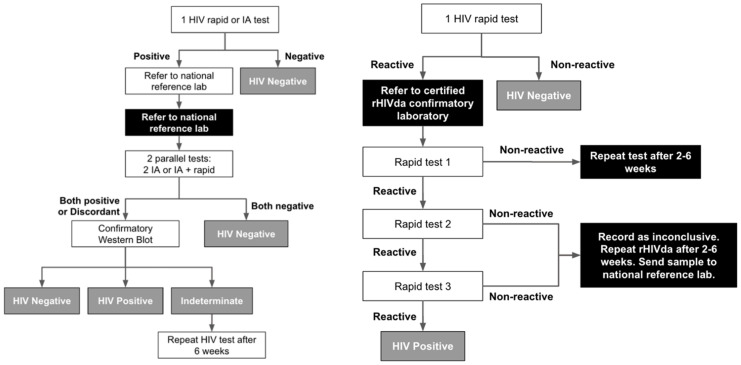
In the past decade, the Philippines has gained notoriety as the country with the fastest-growing human immunodeficiency virus (HIV) epidemic in the Western Pacific region. While the overall trends of HIV incidence and acquired immunodeficiency syndrome (AIDS)-related deaths are declining globally, an increase in new cases was reported to the HIV/AIDS and ART Registry of the Philippines. From 2012 to 2023, there was a 411% increase in daily incidence. Late presentation in care remains a concern, with 29% of new confirmed HIV cases in January 2023 having clinical manifestations of advanced HIV disease at the time of diagnosis. Men having sex with men (MSM) are disproportionately affected. Various steps have been taken to address the HIV epidemic in the country. The Philippine HIV and AIDS Policy Act of 2018 (Republic Act 11166) expanded access to HIV testing and treatment. HIV testing now allows for the screening of minors 15-17 years old without parental consent. Community-based organizations have been instrumental in expanding HIV screening to include self-testing and community-based screening. The Philippines moved from centralized HIV diagnosis confirmation by Western blot to a decentralized rapid HIV diagnostic algorithm (rHIVda). Dolutegravir-based antiretroviral therapy is now the first line. Pre-exposure prophylaxis in the form of emtricitabine-tenofovir disoproxil fumarate has been rolled out. The number of treatment hubs and primary HIV care facilities continues to increase. Despite these efforts, barriers to ending the HIV epidemic remain, including continued stigma, limited harm reduction services for people who inject drugs, sociocultural factors, and political deterrents. HIV RNA quantification and drug resistance testing are not routinely performed due to associated costs. The high burden of tuberculosis and hepatitis B virus co-infection complicate HIV management. CRF_01AE is now the predominant subtype, which has been associated with poorer clinical outcomes and faster CD4 T-cell decline. The HIV epidemic in the Philippines requires a multisectoral approach and calls for sustained political commitment, community involvement, and continued collaboration among various stakeholders. In this article, we outline the current progress and challenges in curbing the HIV epidemic in the Philippines.
在过去十年中,菲律宾因成为西太平洋地区人类免疫缺陷病毒(HIV)疫情增长最快的国家而声名狼藉。虽然全球HIV发病率和获得性免疫缺陷综合征(AIDS)相关死亡的总体趋势在下降,但菲律宾HIV/AIDS和抗逆转录病毒治疗登记处报告新病例有所增加。2012年至2023年,日发病率增长了411%。护理延迟就诊仍是一个问题,2023年1月新确诊的HIV病例中有29%在诊断时已出现晚期HIV疾病的临床表现。男男性行为者(MSM)受影响尤为严重。该国已采取各种措施应对HIV疫情。2018年的《菲律宾HIV和AIDS政策法案》(第11166号共和国法案)扩大了HIV检测和治疗的可及性。现在HIV检测允许在未经父母同意的情况下对15至17岁的未成年人进行筛查。社区组织在扩大HIV筛查范围以包括自我检测和社区筛查方面发挥了重要作用。菲律宾从通过蛋白印迹法进行集中HIV诊断确认转变为分散式快速HIV诊断算法(rHIVda)。基于多替拉韦的抗逆转录病毒疗法现在是一线治疗方案。已推出以恩曲他滨替诺福韦酯形式的暴露前预防措施。治疗中心和初级HIV护理设施的数量持续增加。尽管做出了这些努力,但结束HIV疫情的障碍仍然存在,包括持续的耻辱感、针对注射吸毒者的减少伤害服务有限、社会文化因素和政治阻碍。由于相关成本,HIV RNA定量和耐药性检测未常规开展。结核病和乙型肝炎病毒合并感染的高负担使HIV管理复杂化。CRF_01AE现在是主要亚型,这与较差的临床结果和更快的CD4 T细胞下降有关。菲律宾的HIV疫情需要多部门方法,并需要持续的政治承诺、社区参与以及各利益相关方之间的持续合作。在本文中,我们概述了菲律宾在遏制HIV疫情方面的当前进展和挑战。