US Health Outcomes, GlaxoSmithKline, Research Triangle Park, NC 27709, USA.
Int J Chron Obstruct Pulmon Dis. 2010 Dec 31;6:13-22. doi: 10.2147/COPD.S15455.
Relative costs and utilization-related outcomes of a fluticasone propionate 250 μg + salmeterol 50 μg combination (FSC), tiotropium bromide, and ipratropium as initial maintenance therapy in COPD have not been compared in a commercially-insured population.
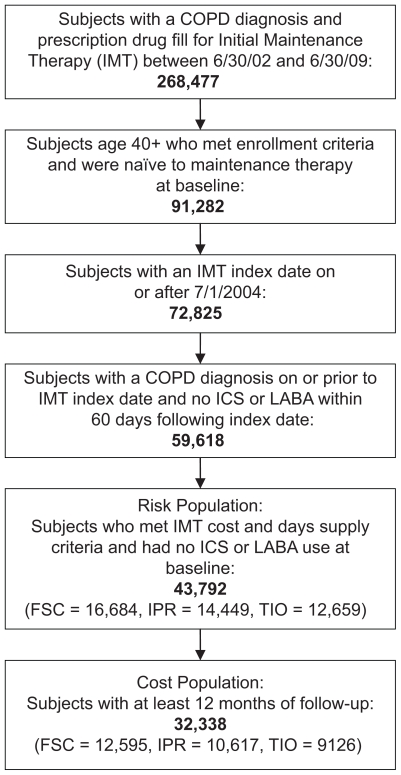
This retrospective, observational cohort study used health care claims data from January 2004 to June 2009 from a large administrative database for patients aged ≥40 years with COPD. Time-to-first COPD-related health care event beginning 30 days following therapy initiation with FSC (n = 16,684), ipratropium alone or in fixed dose combination with albuterol (n = 14,449), or tiotropium (n = 12,659) was estimated using Cox proportional hazard models that controlled for differences in patient demographic characteristics, health care utilization, and comorbidities at baseline. Mean adjusted costs and numbers of COPD-related health care encounters and prescription medication fills were compared among patients with 12 months of follow-up (FSC, n = 12,595; ipratropium, n = 10,617; tiotropium, n = 9126).
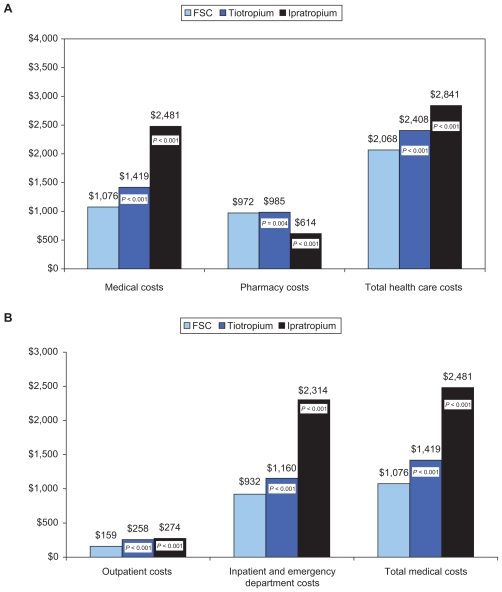
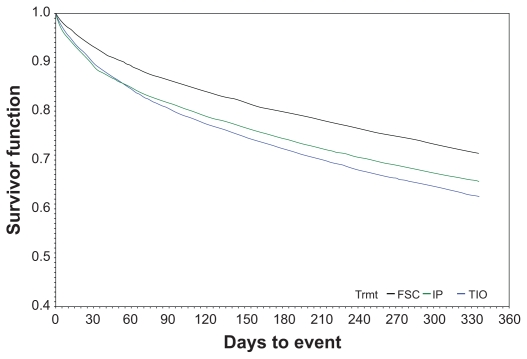
With FSC as the reference, risk for a COPD-related hospitalization and/or emergency department visit was significantly higher for ipratropium (hazard ratio [HR] 1.64, 95% confidence interval [CI] 1.50-1.79) and tiotropium (HR 1.29, CI 1.17-1.41). Mean adjusted 12-month COPD-related total health care costs were lower for FSC ($2068, standard deviation [SD] $1190) than for ipratropium ($2841, SD $1858) and tiotropium ($2408, SD $1511, both P <0.05). Mean number of COPD-related hospitalizations, emergency department visits, and outpatient visits associated with an oral corticosteroid or antibiotic were also lower for FSC than for ipratropium and tiotropium (all P <0.05).
In this retrospective "real-world" observational sample of COPD patients, initiating treatment with FSC was associated with significantly better clinical and economic outcomes compared with short- and long-acting anticholinergic therapy. Consistent with the goal of preventing and reducing exacerbations advocated by global guidelines, the findings suggest that initiation of maintenance treatment with FSC may afford clinical benefits at a lower cost than anticholinergic treatment.
在商业保险人群中,尚未比较丙酸氟替卡松 250μg+沙美特罗 50μg 联合制剂(FSC)、噻托溴铵和异丙托溴铵作为 COPD 初始维持治疗的相对成本和与利用相关的结果。
本回顾性观察性队列研究使用了来自大型行政数据库的 2004 年 1 月至 2009 年 6 月期间年龄≥40 岁的 COPD 患者的医疗保健索赔数据。使用 Cox 比例风险模型估算自治疗开始后 30 天开始的首次 COPD 相关医疗保健事件的时间(FSC 组 n=16684,异丙托铵单独或与沙丁胺醇固定剂量联合使用组 n=14449,噻托溴铵组 n=12659),该模型控制了患者人口统计学特征、医疗保健利用和基线合并症的差异。在有 12 个月随访的患者中比较了 FSC(n=12595)、异丙托铵(n=10617)和噻托溴铵(n=9126)的平均调整后 COPD 相关医疗保健费用和 COPD 相关医疗保健次数和处方药物用量。
以 FSC 为参照,与异丙托铵(风险比 [HR] 1.64,95%置信区间 [CI] 1.50-1.79)和噻托溴铵(HR 1.29,CI 1.17-1.41)相比,FSC 治疗的 COPD 相关住院和/或急诊就诊风险显著更高。FSC 的平均调整后 12 个月 COPD 相关总医疗保健费用低于异丙托铵(2841 美元,标准偏差 [SD] 1858 美元)和噻托溴铵(2408 美元,SD 1511 美元,均 P<0.05)。FSC 相关的 COPD 相关住院、急诊就诊和门诊就诊次数也低于异丙托铵和噻托溴铵,需要口服皮质激素或抗生素治疗(均 P<0.05)。
在这项 COPD 患者的回顾性“真实世界”观察性样本中,与短期和长效抗胆碱能药物治疗相比,用 FSC 起始治疗与显著更好的临床和经济结果相关。与全球指南倡导的预防和减少恶化的目标一致,这些发现表明,与抗胆碱能治疗相比,用 FSC 起始维持治疗可能具有更低的成本和更好的临床获益。