Vrije Universiteit Medical Centre, Department of Intensive Care, De Boelelaan 1117, 1081 HV Amsterdam, The Netherlands.
Crit Care. 2011;15(1):R73. doi: 10.1186/cc10062. Epub 2011 Feb 25.
Static cardiac filling volumes have been suggested to better predict fluid responsiveness than filling pressures, but this may not apply to hearts with systolic dysfunction and dilatation. We evaluated the relative value of cardiac filling volume and pressures for predicting and monitoring fluid responsiveness, according to systolic cardiac function, estimated by global ejection fraction (GEF, normal 25 to 35%) from transpulmonary thermodilution.
We studied hypovolemic, mechanically ventilated patients after coronary (n = 18) or major vascular (n = 14) surgery in the intensive care unit. We evaluated 96 colloid fluid loading events (200 to 600 mL given in three consecutive 30-minute intervals, guided by increases in filling pressures), divided into groups of responding events (fluid responsiveness) and non-responding events, in patients with low GEF (<20%) or near-normal GEF (≥ 20%). Patients were monitored by transpulmonary dilution and central venous (n = 9)/pulmonary artery (n = 23) catheters to obtain cardiac index (CI), global end-diastolic volume index (GEDVI), central venous (CVP) and pulmonary artery occlusion pressure (PAOP).
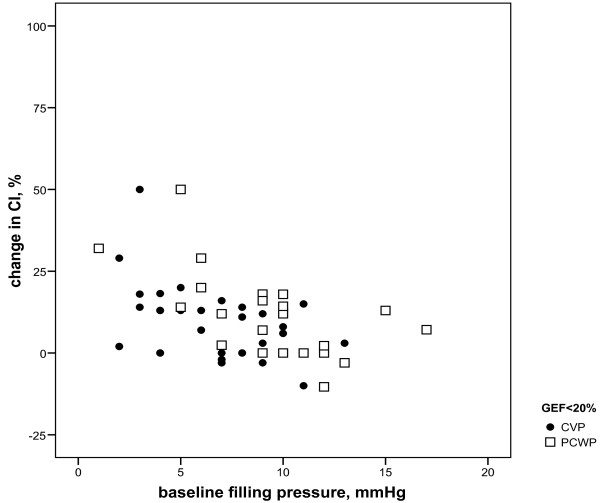
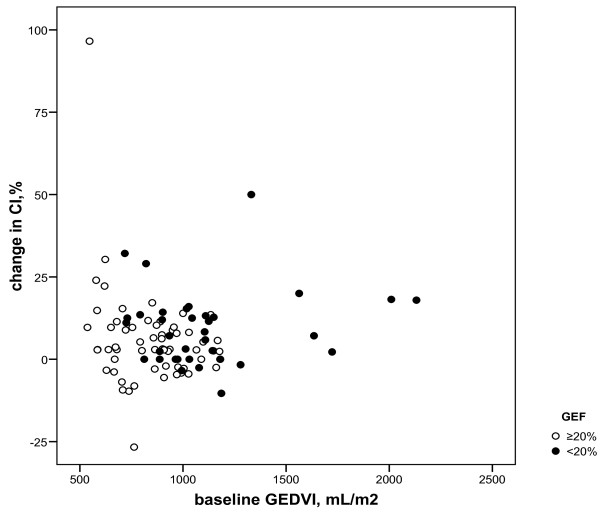
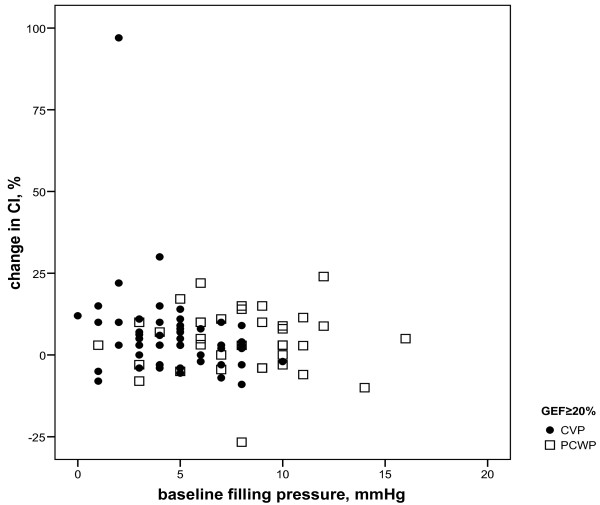
Fluid responsiveness occurred in 8 (≥ 15% increase in CI) and 17 (≥ 10% increase in CI) of 36 fluid loading events when GEF was <20%, and 7 (≥ 15% increase in CI) and 17 (≥ 10% increase in CI) of 60 fluid loading events when GEF was ≥ 20%. Whereas a low baseline GEDVI predicted fluid responsiveness particularly when GEF was ≥ 20% (P = 0.002 or lower), a low PAOP was of predictive value particularly when GEF was <20% (P = 0.004 or lower). The baseline CVP was lower in responding events regardless of GEF. Changes in CVP and PAOP paralleled changes in CI particularly when GEF was <20%, whereas changes in GEDVI paralleled CI regardless of GEF.
Regardless of GEF, CVP may be useful for predicting fluid responsiveness in patients after coronary and major vascular surgery provided that positive end-expiratory pressure is low. When GEF is low (<20%), PAOP is more useful than GEDVI for predicting fluid responsiveness, but when GEF is near-normal (≥20%) GEDVI is more useful than PAOP. This favors predicting and monitoring fluid responsiveness by pulmonary artery catheter-derived filling pressures in surgical patients with systolic left ventricular dysfunction and by transpulmonary thermodilution-derived GEDVI when systolic left ventricular function is relatively normal.
与充盈压相比,静态心脏充盈量被认为可以更好地预测液体反应性,但这可能不适用于伴有收缩功能障碍和扩张的心脏。我们根据经肺热稀释法估计的整体射血分数(GEF,正常 25 至 35%)评估了心脏充盈量和压力对预测和监测液体反应性的相对价值。
我们研究了冠状动脉(n=18)或大血管手术后(n=14)在重症监护病房中出现低血容量的机械通气患者。我们评估了 96 次胶体液负荷事件(分为 3 个 30 分钟的连续间隔,以充盈压增加为指导,给予 200 至 600ml),分为反应性事件(液体反应性)和非反应性事件组,患者的 GEF 较低(<20%)或接近正常(≥20%)。通过经肺稀释和中心静脉(n=9)/肺动脉(n=23)导管监测心指数(CI)、全心舒张末期容积指数(GEDVI)、中心静脉压(CVP)和肺动脉闭塞压(PAOP)。
当 GEF<20%时,8(CI 增加≥15%)和 17(CI 增加≥10%)个液体负荷事件发生液体反应性,当 GEF≥20%时,7(CI 增加≥15%)和 17(CI 增加≥10%)个液体负荷事件发生液体反应性。基线 GEDVI 较低可预测液体反应性,特别是当 GEF≥20%时(P=0.002 或更低),而基线 PAOP 较低则具有预测价值,特别是当 GEF<20%时(P=0.004 或更低)。无论 GEF 如何,反应性事件的基线 CVP 均较低。CVP 和 PAOP 的变化与 CI 的变化特别相关,特别是当 GEF<20%时,而 GEDVI 的变化与 CI 无关,无论 GEF 如何。
无论 GEF 如何,只要呼气末正压较低,CVP 可用于预测冠状动脉和大血管手术后患者的液体反应性。当 GEF 较低(<20%)时,PAOP 比 GEDVI 更有助于预测液体反应性,但当 GEF 接近正常(≥20%)时,GEDVI 比 PAOP 更有用。这有利于在伴有收缩性左心室功能障碍的外科患者中通过肺动脉导管衍生的充盈压和在收缩性左心室功能相对正常的情况下通过经肺热稀释衍生的 GEDVI 来预测和监测液体反应性。