Intensive Care Department, Hospital Universitario de Getafe, Getafe, Madrid, Spain.
Intensive Care Med. 2011 May;37(5):768-74. doi: 10.1007/s00134-011-2167-7. Epub 2011 Mar 11.
To describe the incidence, risk factors, and impact on mortality of acute kidney injury (AKI) in patients with 2009 influenza A (H1N1) viral pneumonia requiring mechanical ventilation.
Observational cohort study.
AKI was defined as risk, injury or failure, according to the RIFLE classification. Early and late AKI were defined as AKI occurring on intensive care unit (ICU) day 2 or before, or after ICU day 2, respectively. Demographic data and information on organ dysfunction were collected daily.
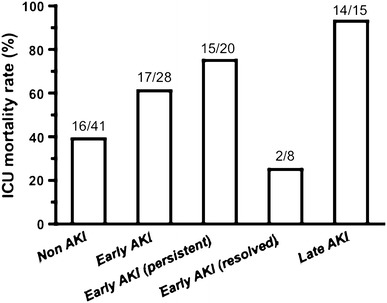
Of 84 patients, AKI developed in 43 patients (51%). Twenty (24%) needed renal replacement therapy. Early and late AKI were found in 28 (33%) and 15 (18%) patients, respectively. Patients with AKI, as compared with patients without AKI, had higher Acute Physiology and Chronic Health Evaluation (APACHE) II score and ICU mortality (72% versus 39%, p < 0.01) and presented on admission more marked cardiovascular, respiratory, and hematological dysfunction. Patients with early but not late AKI presented on admission higher APACHE II score and more marked organ dysfunction, as compared with patients without AKI. ICU mortality was higher in late versus early AKI (93% versus 61%, p < 0.001). On multivariate analysis, only APACHE II score and late but not early AKI [odds ratio (OR) 1.1 (95% confidence interval 1.0-1.1) and 15.1 (1.8-130.7), respectively] were associated with mortality.
AKI is a frequent complication of 2009 influenza A (H1N1) viral pneumonia. AKI developing after 2 days in ICU appears to be associated with different risk factors than early AKI, and is related to a higher mortality rate.
描述需要机械通气的 2009 年甲型 H1N1 流感病毒性肺炎患者中急性肾损伤(AKI)的发生率、危险因素和对死亡率的影响。
观察性队列研究。
根据 RIFLE 分类,将 AKI 定义为风险、损伤或衰竭。早期和晚期 AKI 分别定义为发生在重症监护病房(ICU)第 2 天或之前和之后的 AKI。每天收集人口统计学数据和器官功能障碍信息。
在 84 例患者中,43 例(51%)发生 AKI。20 例(24%)需要肾脏替代治疗。28 例(33%)和 15 例(18%)患者分别发生早期和晚期 AKI。与无 AKI 的患者相比,AKI 患者的急性生理学和慢性健康评估(APACHE)Ⅱ评分和 ICU 死亡率更高(72%比 39%,p<0.01),入院时心血管、呼吸和血液系统功能障碍更为明显。与无 AKI 的患者相比,早期 AKI 患者入院时的 APACHEⅡ评分和器官功能障碍更为明显,但晚期 AKI 患者则不然。与早期 AKI 相比,晚期 AKI 的 ICU 死亡率更高(93%比 61%,p<0.001)。多变量分析显示,只有 APACHEⅡ评分和晚期而非早期 AKI(比值比 1.1(95%置信区间 1.0-1.1)和 15.1(1.8-130.7))与死亡率相关。
AKI 是 2009 年甲型 H1N1 流感病毒性肺炎的常见并发症。在 ICU 后 2 天发生的 AKI 似乎与早期 AKI 有不同的危险因素有关,与更高的死亡率相关。