Madras Diabetes Research Foundation & Dr Mohan's Diabetes Specialities Centre, WHO Collaborating Centre for Non-Communicable Diseases Prevention & Control, International Diabetes Federation Centre of Education, Chennai, India.
Indian J Med Res. 2011 Mar;133(3):294-9.
BACKGROUND & OBJECTIVES: With increasing number of people with diabetes worldwide, particularly in India, it is necessary to search for low cost screening methods. We compared the effectiveness and costs of screening for undiagnosed type 2 diabetes mellitus (T2DM), using oral glucose tolerance testing (OGTT) alone, or following a positive result from the Indian Diabetes Risk Score (IDRS) or following a positive result from genotyping of the TCF7L2 polymorphisms in Asian Indians.
In subjects without known diabetes (n=961) recruited from the Chennai Urban Rural Epidemiology Study (CURES), OGTT, IDRS, and genotyping of rs12255372 (G/T) and rs7903146(C/T) of TCF7L2 polymorphisms were done. IDRS includes four parameters: age, abdominal obesity, family history of T2DM and physical activity.
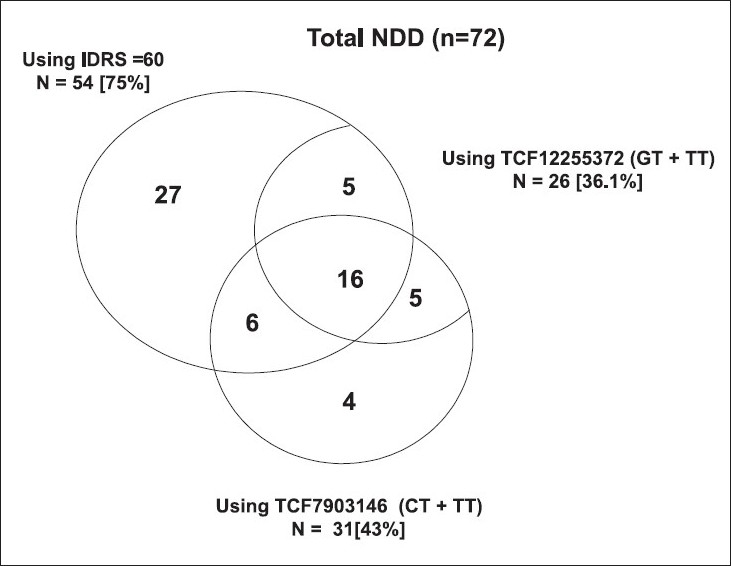
OGTT identified 72 subjects with newly diagnosed diabetes (NDD), according to the World Health Organization criteria of fasting plasma glucose ≥ 126 mg/dl or a plasma glucose ≥ 200 mg/dl, 2 h after 75 g oral glucose load. IDRS screening (cut-off ≥ 60) yielded 413 positive subjects, which included 54 (75%) of the 72 NDD subjects identified by OGTT. Genotyping yielded 493 positive subjects which only included 36 (50%) of the 72 NDD subjects showing less discriminatory power. Screening with both SNPs missed 27 (37.5%) NDD subjects identified by IDRS. In contrast, IDRS missed only 9 (12.5%) of the NDD subjects identified by genotyping. Total screening cost for OGTT alone, or with IDRS were rs 384,400 and 182,810 respectively. Comparing OGTT alone to IDRS followed by OGTT, the incremental cost per additional NDD subject detected by doing OGTT on everyone was rs 11,199 (rs 201,590 for detecting additional 18 NDD subjects).
INTERPRETATION & CONCLUSIONS: For screening a population of subjects without diagnosed diabetes in India, a simple diabetes risk score is more effective and less expensive than genotyping or doing OGTT on the whole population.
随着全球糖尿病患者数量的增加,特别是在印度,有必要寻找低成本的筛查方法。我们比较了单独使用口服葡萄糖耐量试验(OGTT)、印度糖尿病风险评分(IDRS)阳性结果或亚洲印度人 TCF7L2 多态性基因分型阳性结果筛查未确诊的 2 型糖尿病(T2DM)的有效性和成本。
在从 Chennai Urban Rural Epidemiology Study(CURES)招募的 961 名无已知糖尿病的受试者中,进行 OGTT、IDRS 和 TCF7L2 多态性 rs12255372(G/T)和 rs7903146(C/T)的基因分型。IDRS 包括四个参数:年龄、腹部肥胖、2 型糖尿病家族史和体力活动。
根据世界卫生组织空腹血糖≥126mg/dl 或口服 75g 葡萄糖后 2h 血糖≥200mg/dl 的标准,OGTT 确定了 72 名新诊断为糖尿病(NDD)的患者。IDRS 筛查(截断值≥60)共筛查出 413 例阳性病例,其中包括 54 例(75%)OGTT 筛查出的 72 例 NDD 患者。基因分型共筛查出 493 例阳性病例,其中仅包括 36 例(50%)OGTT 筛查出的 72 例 NDD 患者,因此具有较低的判别能力。筛查这两种 SNP 共漏诊了 27 例(37.5%)IDRS 筛查出的 NDD 患者。相比之下,IDRS 仅漏诊了 9 例(12.5%)由基因分型筛查出的 NDD 患者。单独进行 OGTT 筛查或结合 IDRS 筛查的总筛查成本分别为 384400 卢比和 182810 卢比。与单独进行 OGTT 相比,对每个人进行 OGTT 后,通过 IDRS 发现额外 NDD 患者的增量成本为 11199 卢比(发现额外 18 例 NDD 患者的成本为 201590 卢比)。
对于筛查印度无确诊糖尿病的人群,简单的糖尿病风险评分比基因分型或对整个人群进行 OGTT 更有效且成本更低。