Division of Infectious Diseases, CHU St-Pierre, Université Libre de Bruxelles, Brussels, Belgium.
J Int AIDS Soc. 2011 Mar 28;14:16. doi: 10.1186/1758-2652-14-16.
Non-AIDS-defining malignancies (NADM) are becoming a major cause of mortality in the era of highly active antiretroviral therapy. We wished to investigate the incidence, risks factors and outcome of NADM in an urban cohort.
We carried out an observational cohort of HIV patients with 12,746 patient-years of follow up between January 2002 and March 2009. Socio-demographics and clinical characteristics of patients diagnosed with NADM were retrospectively compared with the rest of the cohort. Causes of death and risk factors associated with NADM were assessed using logistic regression. Survival analyses were performed with Kaplan-Meier estimates. Cancer incidences were compared with those of the general population of the Brussels-Capital Region using the standardized incidence ratio (SIR).
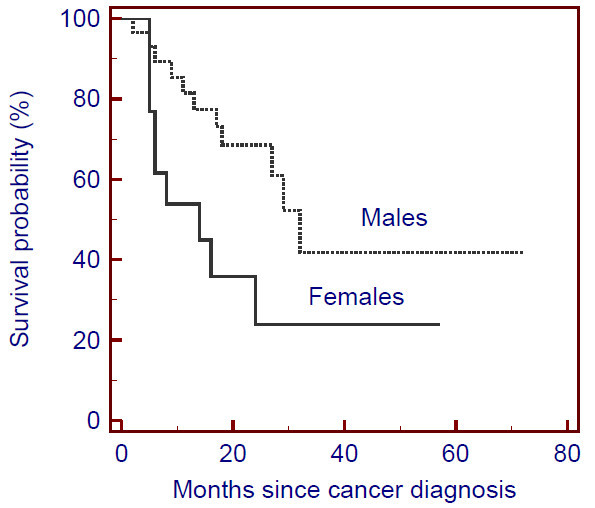
Forty-five NADM were diagnosed. At inclusion in the study, patients with NADM were older than patients without NADM (47 years vs. 38 years, p < 0.001), had a longer history of HIV infection (59 months vs. 39 months, p = 0.0174), a lower nadir CD4 count (110 cells/mm3 vs. 224 cells/mm3, p < 0.0001) and a higher rate of previous AIDS events (33% vs. 20%, p = 0.0455) and of hepatitis C virus co-infection (22.2% vs. 10%, p = 0.0149). In multivariate analysis, age over 45 at baseline (OR 3.25; 95% CI 1.70-6.22) and a nadir CD4 count of less than 200 cells/mm3 (OR 3.10; 95% CI 1.40-6.87) were associated with NADM. NADM were independently associated with higher mortality in the cohort (OR 14.79; 95% CI 6.95-31.49). Women with cancer, the majority of whom were of sub-Saharan African origin, had poorer survival compared with men. The SIR for both sexes were higher than expected for Hodgkin's lymphoma (17.78; 95% CI 6.49-38.71), liver cancers (8.73; 95% CI 2.35-22.34), anal cancers (22.67; 95% CI 8.28-49.34) and bladder cancers (3.79; 95% CI 1.02-9.70). The SIR for breast cancer was lower in women (SIR 0.29; 95% CI 0.06-0.85).
Age over 45 and a nadir CD4 count of less than 200 cells/mm3 were predictive of NADM in our cohort. Mortality was high, especially in sub-Saharan African women. Cancers with increased incidences were Hodgkin's lymphoma and anal, bladder and liver cancers in both sexes; women had a lower incidence of breast cancer.
在高效抗逆转录病毒治疗时代,非艾滋病定义性恶性肿瘤(NADM)成为导致死亡的主要原因。我们希望在城市队列中研究 NADM 的发病率、风险因素和结局。
我们对 2002 年 1 月至 2009 年 3 月期间接受了 12746 患者年随访的 HIV 患者进行了一项观察性队列研究。回顾性比较了诊断为 NADM 的患者与队列中其余患者的社会人口统计学和临床特征。使用逻辑回归评估 NADM 的死亡原因和相关风险因素。采用 Kaplan-Meier 估计法进行生存分析。使用标准化发病比(SIR)比较癌症发病率与布鲁塞尔首都大区的一般人群。
诊断出 45 例 NADM。在纳入研究时,患有 NADM 的患者比没有 NADM 的患者年龄更大(47 岁比 38 岁,p < 0.001),HIV 感染史更长(59 个月比 39 个月,p = 0.0174),CD4 计数最低值更低(110 个细胞/mm3 比 224 个细胞/mm3,p < 0.0001),且既往 AIDS 事件发生率更高(33%比 20%,p = 0.0455)和丙型肝炎病毒合并感染率更高(22.2%比 10%,p = 0.0149)。多变量分析显示,基线时年龄超过 45 岁(OR 3.25;95%CI 1.70-6.22)和 CD4 计数最低值低于 200 个细胞/mm3(OR 3.10;95%CI 1.40-6.87)与 NADM 相关。NADM 与队列中的高死亡率独立相关(OR 14.79;95%CI 6.95-31.49)。患有癌症的女性,其中大多数来自撒哈拉以南非洲,与男性相比生存率更差。男性和女性的 SIR 均高于预期,其中 Hodgkin 淋巴瘤(17.78;95%CI 6.49-38.71)、肝癌(8.73;95%CI 2.35-22.34)、肛门癌(22.67;95%CI 8.28-49.34)和膀胱癌(3.79;95%CI 1.02-9.70)的 SIR 更高。女性的乳腺癌 SIR 较低(SIR 0.29;95%CI 0.06-0.85)。
在我们的队列中,年龄超过 45 岁和 CD4 计数最低值低于 200 个细胞/mm3 是 NADM 的预测因素。死亡率很高,尤其是撒哈拉以南非洲裔女性。发病率增加的癌症包括两性的霍奇金淋巴瘤和肛门、膀胱和肝脏癌症;女性乳腺癌的发病率较低。