Nijmegen Institute for International Health, Radboud University Nijmegen Medical Centre, Nijmegen, the Netherlands.
Malar J. 2011 Apr 2;10:76. doi: 10.1186/1475-2875-10-76.
Patterns of decreasing malaria transmission intensity make presumptive treatment of malaria an unjustifiable approach in many African settings. The controlled use of anti-malarials after laboratory confirmed diagnosis is preferable in low endemic areas. Diagnosis may be facilitated by malaria rapid diagnostic tests (RDTs). In this study, the impact of a government policy change, comprising the provision of RDTs and advice to restrict anti-malarial treatment to RDT-positive individuals, was assessed by describing diagnostic behaviour and treatment decision-making in febrile outpatients <10 years of age in three hospitals in the Kagera and Mwanza Region in northern Tanzania.
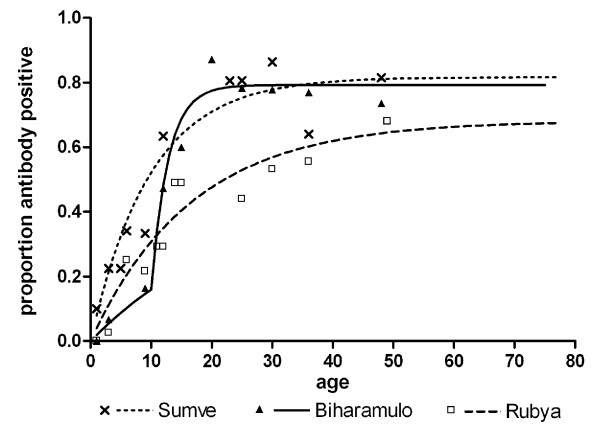
Prospective data from Biharamulo and Rubya Designated District Hospital (DDH) were collected before and after policy change, in Sumve DDH no new policy was implemented. Diagnosis of malaria was confirmed by RDT; transmission intensity was evaluated by a serological marker of malaria exposure in hospital attendees.
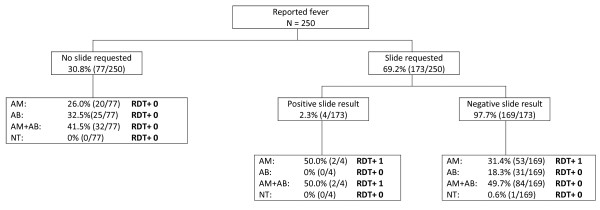
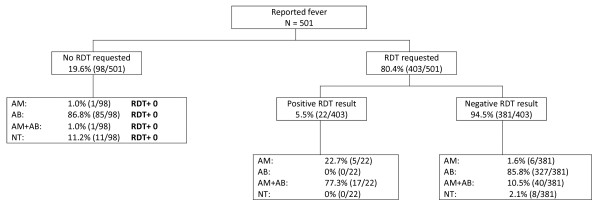
Prior to policy change, there was no evident association between the actual level of transmission intensity and drug-prescribing behaviour. After policy change, there was a substantial decrease in anti-malarial prescription and an increase in prescription of antibiotics. The proportion of parasite-negative individuals who received anti-malarials decreased from 89.1% (244/274) to 38.7% (46/119) in Biharamulo and from 76.9% (190/247) to 10.0% (48/479) in Rubya after policy change.
This study shows that an official policy change, where RDTs were provided and healthcare providers were advised to adhere to RDT results in prescribing drugs can be followed by more rational drug-prescribing behaviour. The current findings are promising for improving treatment policy in Tanzanian hospitals.
在许多非洲地区,疟疾传播强度降低的模式使得疟疾的推定治疗成为不合理的方法。在低流行地区,最好在实验室确诊后使用抗疟药物进行有控制的使用。疟疾快速诊断检测(RDT)可以帮助诊断。在这项研究中,通过描述在坦桑尼亚北部卡盖拉和姆万扎地区的三家医院发热门诊 10 岁以下患者的诊断行为和治疗决策,评估了一项政府政策变化的影响,该政策变化包括提供 RDT 和建议将抗疟药物治疗限制在 RDT 阳性个体。
在政策变化前后,从比哈罗和鲁巴指定区医院(DDH)收集前瞻性数据,在 Sumve DDH 没有实施新政策。疟疾诊断通过 RDT 确认;通过医院就诊者的疟疾暴露血清学标志物评估传播强度。
在政策变化之前,实际传播强度和药物处方行为之间没有明显的关联。政策变化后,抗疟药物的处方大量减少,抗生素的处方增加。寄生虫阴性个体接受抗疟药物的比例从比哈罗的 89.1%(244/274)降至 38.7%(46/119),从鲁巴的 76.9%(190/247)降至 10.0%(48/479)。
这项研究表明,官方政策的改变,即提供 RDT 并建议医疗保健提供者遵守 RDT 结果以开具药物,可以导致更合理的药物处方行为。目前的发现有望改善坦桑尼亚医院的治疗政策。