Centre for Virology, UCL Medical School, London, UK.
Lancet. 2011 Apr 9;377(9773):1256-63. doi: 10.1016/S0140-6736(11)60136-0.
Cytomegalovirus end-organ disease can be prevented by giving ganciclovir when viraemia is detected in allograft recipients. Values of viral load correlate with development of end-organ disease and are moderated by pre-existing natural immunity. Our aim was to determine whether vaccine-induced immunity could do likewise.
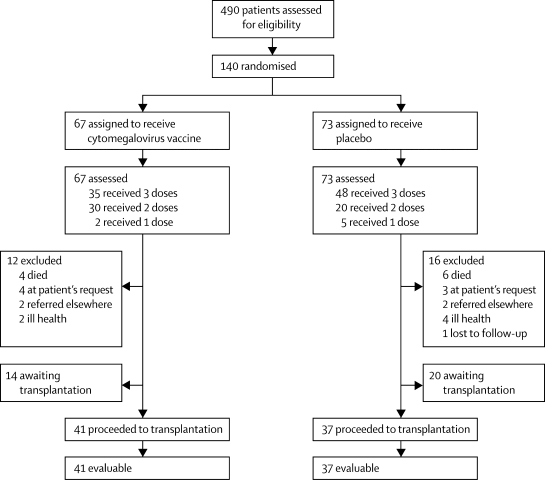
We undertook a phase-2 randomised placebo controlled trial in adults awaiting kidney or liver transplantation at the Royal Free Hospital, London, UK. Exclusion criteria were pregnancy, receipt of blood products (except albumin) in the previous 3 months, and simultaneous multiorgan transplantation. 70 patients seronegative and 70 seropositive for cytomegalovirus were randomly assigned from a scratch-off randomisation code in a 1:1 ratio to receive either cytomegalovirus glycoprotein-B vaccine with MF59 adjuvant or placebo, each given at baseline, 1 month and 6 months later. If a patient was transplanted, no further vaccinations were given and serial blood samples were tested for cytomegalovirus DNA by real-time quantitative PCR (rtqPCR). Any patient with one blood sample containing more than 3000 cytomegalovirus genomes per mL received ganciclovir until two consecutive undetectable cytomegalovirus DNA measurements. Safety and immunogenicity were coprimary endpoints and were assessed by intention to treat in patients who received at least one dose of vaccine or placebo. This trial is registered with ClinicalTrials.gov, NCT00299260.
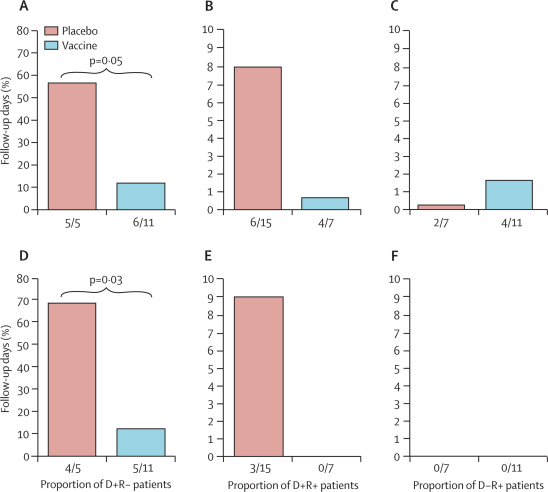
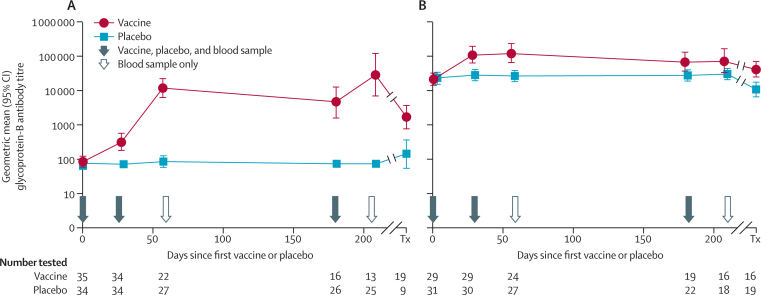
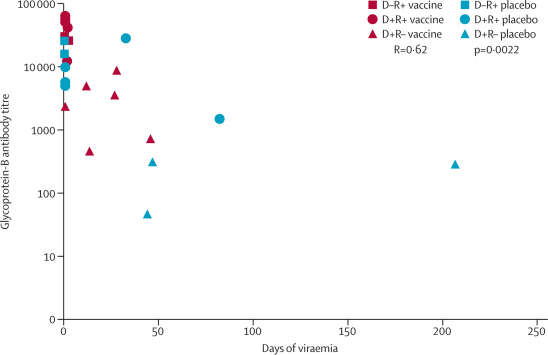
67 patients received vaccine and 73 placebo, all of whom were evaluable. Glycoprotein-B antibody titres were significantly increased in both seronegative (geometric mean titre 12,537 (95% CI 6593-23,840) versus 86 (63-118) in recipients of placebo recipients; p<0.0001) and seropositive (118,395; 64,503-217,272) versus 24,682 (17,909-34,017); p<0.0001) recipients of vaccine. In those who developed viraemia after transplantation, glycoprotein-B antibody titres correlated inversely with duration of viraemia (p=0.0022). In the seronegative patients with seropositive donors, the duration of viraemia (p=0.0480) and number of days of ganciclovir treatment (p=0.0287) were reduced in vaccine recipients.
Although cytomegalovirus disease occurs in the context of suppressed cell-mediated immunity post-transplantation, humoral immunity has a role in reduction of cytomegalovirus viraemia. Vaccines containing cytomegalovirus glycoprotein B merit further assessment in transplant recipients.
National Institute of Allergy and Infectious Diseases, Grant R01AI051355 and Wellcome Trust, Grant 078332.
University College London (UCL).
巨细胞病毒终末器官疾病可以通过在同种异体受者的病毒血症检测时给予更昔洛韦来预防。病毒载量的值与终末器官疾病的发展相关,并受预先存在的天然免疫的调节。我们的目的是确定疫苗诱导的免疫是否也可以做到这一点。
我们在英国伦敦皇家自由医院进行了一项 2 期、随机、安慰剂对照试验,纳入了等待肾或肝移植的成年人。排除标准为妊娠、在过去 3 个月内接受血液制品(白蛋白除外)以及同时进行多器官移植。70 名巨细胞病毒血清阴性和 70 名巨细胞病毒血清阳性的患者根据划痕随机化代码以 1:1 的比例随机分配接受巨细胞病毒糖蛋白-B 疫苗与 MF59 佐剂或安慰剂,两者均在基线、1 个月和 6 个月时给予。如果患者接受了移植,则不再给予疫苗,并且通过实时定量 PCR(rtqPCR)对连续的血液样本进行巨细胞病毒 DNA 检测。任何患者的一个血液样本中含有超过 3000 个巨细胞病毒基因组/毫升,则给予更昔洛韦,直到两次连续检测到不可检测的巨细胞病毒 DNA 测量值。安全性和免疫原性是主要终点,并在接受至少一剂疫苗或安慰剂的患者中进行意向治疗评估。该试验在 ClinicalTrials.gov 注册,NCT00299260。
67 名患者接受了疫苗,73 名患者接受了安慰剂,所有患者均具有可评估性。在血清阴性(几何平均滴度 12537(95%CI 6593-23840)与安慰剂组(86(63-118))和血清阳性(118395;64503-217272)与安慰剂组(24682(17909-34017))患者中,糖蛋白-B 抗体滴度均显著升高;均<0.0001)。在移植后发生病毒血症的患者中,糖蛋白-B 抗体滴度与病毒血症持续时间呈负相关(p=0.0022)。在血清阴性且供体血清阳性的患者中,病毒血症持续时间(p=0.0480)和更昔洛韦治疗天数(p=0.0287)在疫苗组中减少。
尽管巨细胞病毒疾病发生在移植后细胞介导免疫抑制的背景下,但体液免疫在减少巨细胞病毒病毒血症方面发挥了作用。含有巨细胞病毒糖蛋白 B 的疫苗值得在移植受者中进一步评估。
美国国立过敏和传染病研究所,R01AI051355 拨款和威康信托基金会,078332 拨款。
伦敦大学学院(UCL)。