Lekka Joanna A, Gavresea Theofani V, Stanc-Giannakopoulos Gabriela A, Demertzis Nikolaos S
Department of Pathology, Metaxas Anticancer Hospital, Piraeus, Greece.
J Med Case Rep. 2011 Apr 12;5:145. doi: 10.1186/1752-1947-5-145.
An aneurysmal bone cyst is a benign but often rapidly expanding osteolytic multi-cystic osseous lesion that occurs as a primary, secondary, intra-osseous, extra-osseous, solid or conventional lesion. It frequently coexists with other benign and malignant bone tumors. Although it is considered to be reactive in nature, there is evidence that some aneurysmal bone cysts are true neoplasms. The solid variant of aneurysmal bone cyst is a rare subtype of aneurysmal bone cyst with a preponderance of solid to cystic elements. Such a case affecting the heel, an unusual site, is reported.
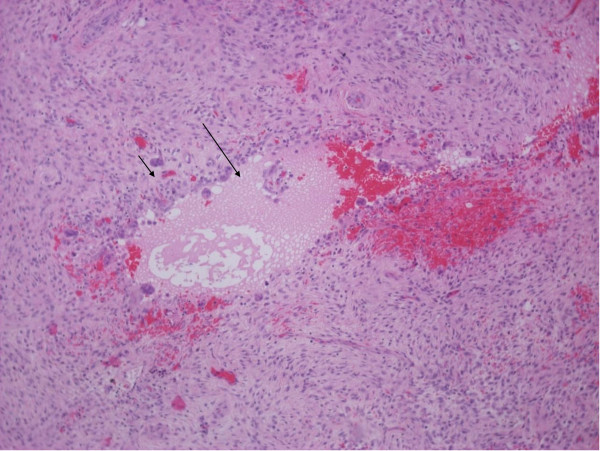
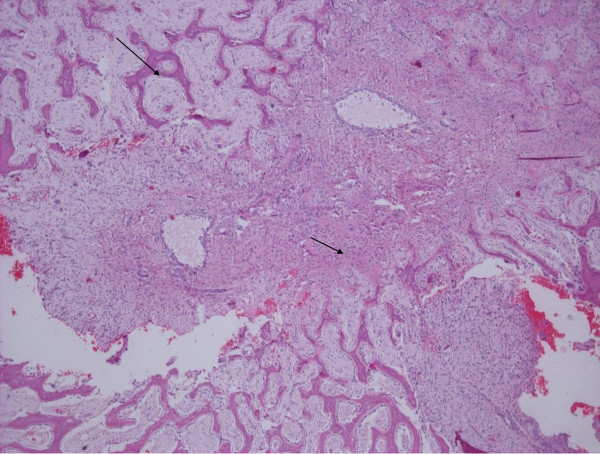
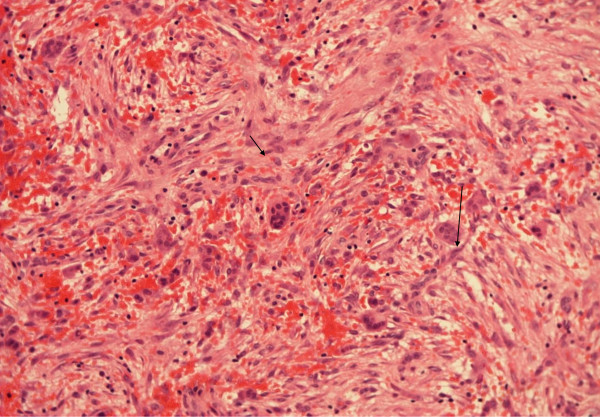
A 26-year-old Caucasian man presented with pain and swelling in his left lower extremity. A plain radiograph demonstrated an intra-osseous, solitary, eccentric mass in the front portion of the left heel. Computed tomography and magnetic resonance imaging scans showed that the lesion appeared to be sub-cortical, solid with a small cystic portion without the characteristic fluid-fluid level detection but with distinct internal septation. Bone images containing fluid-fluid levels are usually produced by aneurysmal bone cysts. The fluid-fluid level due to bleeding within the tumor followed by layering of the blood components based density differences, but it was not seen in our case. An intra-lesional excision was performed. Microscopic examination revealed fibrous septa with spindle cell fibroblastic proliferation, capillaries and extensive areas of mature osteoid and reactive woven bone formation rimmed by osteoblasts. The spindle cells had low mitotic activity, and atypical forms were absent. The histological features of the lesion were consistent with the solid variant of an aneurysmal bone cyst.
Solid aneurysmal bone cysts have been of great interest to pathologists because they may be mistaken for malignant tumors, mainly in cases of giant cell tumors or osteosarcomas, because of cellularity and variable mitotic activity. It is rather obvious that the correlation of clinical, radiological and histological findings is necessary for the differential diagnosis. The eventual diagnosis is based on microscopic evidence and is made when a predominance of solid to cystic elements is found. The present case is of great interest because of the nature of the neoplasm and the extremely unusual location in which it developed. Pathologists must be alert for such a diagnosis.
动脉瘤样骨囊肿是一种良性但通常迅速扩大的溶骨性多囊性骨病变,可表现为原发性、继发性、骨内、骨外、实性或传统性病变。它常与其他良性和恶性骨肿瘤共存。尽管其本质上被认为是反应性的,但有证据表明一些动脉瘤样骨囊肿是真正的肿瘤。动脉瘤样骨囊肿的实性变体是一种罕见的动脉瘤样骨囊肿亚型,实性成分多于囊性成分。本文报道了一例发生在足跟部(一个不常见部位)的此类病例。
一名26岁的白人男性因左下肢疼痛和肿胀前来就诊。X线平片显示左足跟前部有一个骨内、孤立、偏心的肿块。计算机断层扫描和磁共振成像扫描显示,该病变似乎位于皮质下,为实性,有一小部分囊性成分,未检测到特征性的液-液平面,但有明显的内部间隔。含有液-液平面的骨影像通常由动脉瘤样骨囊肿产生。肿瘤内出血导致血液成分根据密度差异分层形成液-液平面,但在我们的病例中未见到。进行了病损内切除。显微镜检查显示纤维间隔,伴有梭形细胞成纤维细胞增生、毛细血管以及广泛的成熟类骨质区域和由成骨细胞包绕的反应性编织骨形成。梭形细胞有低有丝分裂活性,无非典型形态。病变的组织学特征与动脉瘤样骨囊肿的实性变体一致。
实性动脉瘤样骨囊肿一直引起病理学家的极大兴趣,因为它们可能被误诊为恶性肿瘤,主要是在巨细胞瘤或骨肉瘤病例中,原因是细胞丰富和有丝分裂活性可变。显然,临床、放射学和组织学检查结果的相关性对于鉴别诊断是必要的。最终诊断基于显微镜下证据,当发现实性成分多于囊性成分时做出诊断。本病例因其肿瘤性质和发生的极其不寻常位置而极具研究价值。病理学家必须警惕这种诊断。