Kobr Jiri, Fremuth Jiri, Pizingerova Katerina, Sasek Lumir, Jehlicka Petr, Fikrlova Sarka, Slavik Zdenek
Department of Paediatrics, Charles University in Prague, Faculty of Medicine in Pilsen and Faculty Hospital Pilsen, Czech Republic.
Cardiovasc Ultrasound. 2011 Apr 26;9:14. doi: 10.1186/1476-7120-9-14.
The aim of this study was to verify the benefits and limitations of repeated bedside echocardiographic examinations in children during mechanical ventilation. For the purposes of this study, we selected the data of over a time period from 2006 to 2010.
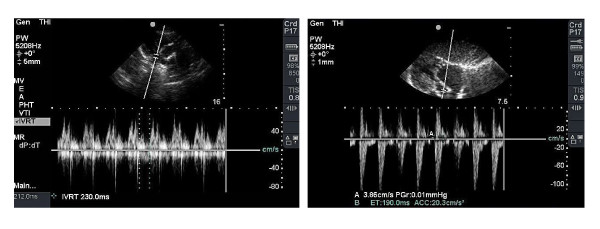
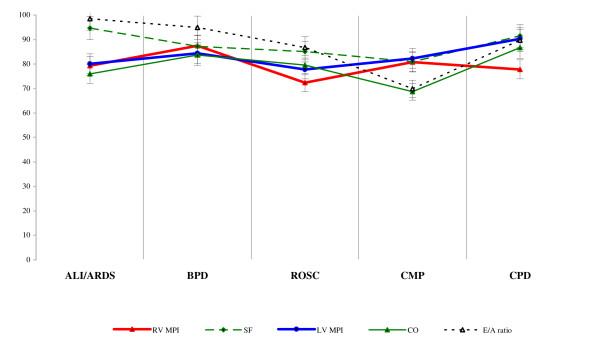
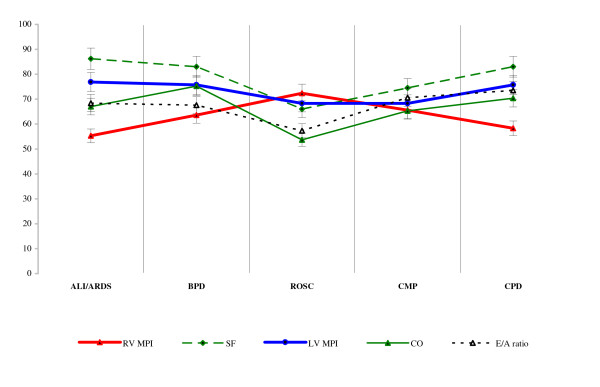
A total of 235 children, average age 3.21 (SD 1.32) years were included into the study and divided into etiopathogenic groups. High-risk groups comprised: Acute lung injury and acute respiratory distress syndrome (ALI/ARDS), return of spontaneous circulation after cardiopulmonary resuscitation (ROSC), bronchopulmonary dysplasia (BPD), cardiomyopathy (CMP) and cardiopulmonary disease (CPD). Transthoracic echocardiography was carried out during mechanical ventilation. The following data were collated for statistical evaluation: right and left ventricle myocardial performance indices (RV MPI; LV MPI), left ventricle shortening fraction (SF), cardiac output (CO), and the mitral valve ratio of peak velocity of early wave (E) to the peak velocity of active wave (A) as E/A ratio. The data was processed after a period of recovery, i.e. one hour after the introduction of invasive lines (time-1) and after 72 hours of comprehensive treatment (time-2). The overall development of parameters over time was compared within groups and between groups using the distribution-free Wilcoxons and two-way ANOVA tests.
A total of 870 echocardiographic examinations were performed. At time-1 higher average values of RV MPI (0.34, SD 0.01 vs. 0.21, SD 0.01; p < 0.001) were found in all groups compared with reference values. Left ventricular load in the high-risk groups was expressed by a higher LV MPI (0.39, SD 0.13 vs. 0.29, SD 0.02; p < 0.01) and lower E/A ratio (0.95, SD 0.36 vs. 1.36, SD 0.64; p < 0.001), SF (0.37, SD 0.11 vs. 0.47, SD 0.02; p < 0.01) and CO (1.95, SD 0.37 vs. 2.94, SD 1.03; p < 0.01). At time-2 RV MPI were lower (0.25, SD 0.02 vs. 0.34, SD 0.01; p < 0.001), but remained higher compared with reference values (0.25, SD 0.02 vs. 0.21, SD 0.01; p < 0.05). Other parameters in high-risk groups were improved, but remained insignificantly different compared with reference values.
Echocardiography complements standard monitoring of valuable information regarding cardiac load in real time. Chest excursion during mechanical ventilation does not reduce the quality of the acquired data.
本研究旨在验证在儿童机械通气期间重复进行床旁超声心动图检查的益处和局限性。为了本研究的目的,我们选取了2006年至2010年期间的一段时间的数据。
共有235名平均年龄为3.21(标准差1.32)岁的儿童纳入本研究,并分为病因组。高危组包括:急性肺损伤和急性呼吸窘迫综合征(ALI/ARDS)、心肺复苏后自主循环恢复(ROSC)、支气管肺发育不良(BPD)、心肌病(CMP)和心肺疾病(CPD)。在机械通气期间进行经胸超声心动图检查。整理以下数据进行统计评估:右心室和左心室心肌性能指标(RV MPI;LV MPI)、左心室缩短分数(SF)、心输出量(CO)以及二尖瓣舒张早期峰值速度(E)与舒张晚期峰值速度(A)之比即E/A比值。在一段时间的恢复后,即插入有创管路1小时后(时间1)和综合治疗72小时后(时间2)对数据进行处理。使用非参数Wilcoxons检验和双向方差分析检验比较组内和组间参数随时间的总体变化情况。
共进行了870次超声心动图检查。在时间1时,与参考值相比,所有组的RV MPI平均值均较高(0.34,标准差0.01对0.21,标准差0.01;p < 0.001)。高危组的左心室负荷表现为较高的LV MPI(0.39,标准差0.13对0.29,标准差0.02;p < 0.01)、较低的E/A比值(0.95,标准差0.36对1.36,标准差0.64;p < 0.001)、SF(0.37,标准差0.11对0.47,标准差0.02;p < 0.01)和CO(1.95,标准差0.37对2.94,标准差1.03;p < 0.01)。在时间2时,RV MPI较低(0.25,标准差0.02对0.34,标准差0.01;p < 0.001),但与参考值相比仍较高(0.25,标准差0.02对0.21,标准差0.01;p < 0.05)。高危组的其他参数有所改善,但与参考值相比仍无显著差异。
超声心动图可实时补充有关心脏负荷的有价值信息的标准监测。机械通气期间的胸廓运动不会降低所获取数据的质量。