Steno Diabetes Center, Gentofte, Denmark.
Diabetes Care. 2011 May;34(5):1081-5. doi: 10.2337/dc10-2459.
To evaluate vitamin D as a predictor of all-cause mortality, progression from normoalbuminuria to micro- or macroalbuminuria, and the development of background or proliferative retinopathy in patients with type 1 diabetes.
A prospective observational follow-up study in which an inception cohort of type 1 diabetic patients was followed from onset of diabetes diagnosed between 1979 and 1984. Plasma vitamin D [25(OH)D3] levels were determined by high performance liquid chromatography/tandem mass spectrometry in 227 patients before the patients developed microalbuminuria. Values equal to or below the 10% percentile (15.5 nmol/L) were considered severe vitamin D deficiency.
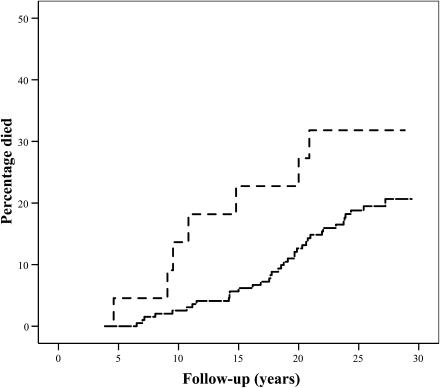
Median (range) vitamin D was 44.6 (1.7-161.7) nmol/L. Vitamin D level was not associated with age, sex, urinary albumin excretion rate (UAER), or blood pressure. During follow-up, 44 (18%) patients died. In a Cox proportional hazards model, the hazard ratio for mortality in subjects with severe vitamin D deficiency was 2.7 (1.1-6.7), P = 0.03, after adjustment for UAER, HbA(1c), and conventional cardiovascular risk factors (age, sex, blood pressure, cholesterol, smoking). Of the 220 patients, 81 (37%) developed microalbuminuria and 27 (12%) of these progressed to macroalbuminuria. Furthermore, 192 (87%) patients developed background retinopathy, whereas 34 (15%) progressed to proliferative retinopathy. Severe vitamin D deficiency at baseline did not predict the development of these microvascular complications.
In patients with type 1 diabetes, severe vitamin D deficiency independently predicts all-cause mortality but not development of microvascular complications in the eye and kidney. Whether vitamin D substitution in type 1 diabetic patients can improve the prognosis remains to be investigated.
评估维生素 D 作为预测全因死亡率、从正常白蛋白尿进展为微量白蛋白尿或大量白蛋白尿以及 1 型糖尿病患者背景性或增殖性视网膜病变发展的指标。
这是一项前瞻性观察性随访研究,其中纳入了 1979 年至 1984 年期间确诊的 1 型糖尿病患者的起始队列,在患者出现微量白蛋白尿之前,通过高效液相色谱/串联质谱法检测 227 例患者的血浆维生素 D [25(OH)D3]水平。维生素 D 水平等于或低于第 10 百分位数(15.5 nmol/L)被认为是严重维生素 D 缺乏。
中位(范围)维生素 D 为 44.6(1.7-161.7)nmol/L。维生素 D 水平与年龄、性别、尿白蛋白排泄率(UAER)或血压无关。在随访期间,44 例(18%)患者死亡。在 Cox 比例风险模型中,严重维生素 D 缺乏患者的死亡风险比为 2.7(1.1-6.7),P = 0.03,在校正 UAER、HbA(1c)和传统心血管危险因素(年龄、性别、血压、胆固醇、吸烟)后。在 220 例患者中,81 例(37%)出现微量白蛋白尿,其中 27 例(12%)进展为大量白蛋白尿。此外,192 例(87%)患者出现背景性视网膜病变,而 34 例(15%)进展为增殖性视网膜病变。基线时严重维生素 D 缺乏并不能预测这些微血管并发症的发生。
在 1 型糖尿病患者中,严重维生素 D 缺乏独立预测全因死亡率,但不能预测眼部和肾脏微血管并发症的发生。1 型糖尿病患者补充维生素 D 是否能改善预后仍有待研究。