International Center for Diarrhoeal Disease Research Bangladesh, Mohakhali, Dhaka, Bangladesh.
PLoS One. 2011 Apr 21;6(4):e18908. doi: 10.1371/journal.pone.0018908.
Malaria is a major public health concern in Bangladesh and it is highly endemic in the Chittagong Hill Tracts where prevalence was 11.7% in 2007. One sub-district, Rajasthali, had a prevalence of 36%. Several interventions were introduced in early 2007 to control malaria. This study was undertaken to evaluate the impacts of these intensive early stage interventions on malaria in Bangladesh. This prevalence study assesses whether or not high malaria prevalence remains, and if so, which areas and individuals remain at high risk of infection.
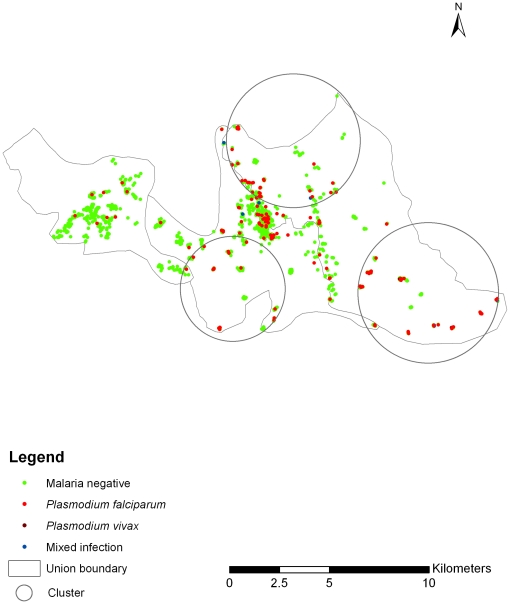
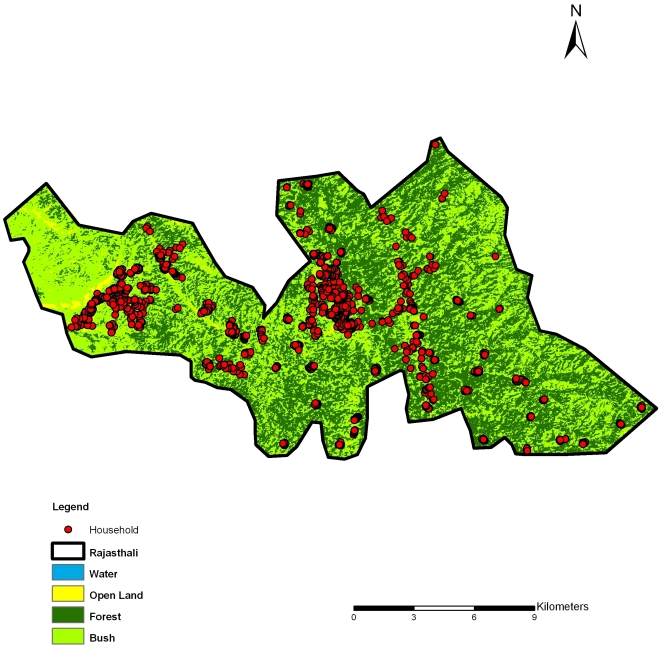
A 2-stage cluster sampling technique was used to sample 1,400 of 5,322 (26.3%) households in Rajasthali, and screened using a rapid diagnostic test (Falci-vax). Overall malaria prevalence was 11.5%. The proportions of Plasmodium falciparum, Plasmodium vivax and infection with both species were 93.2%, 1.9% and 5.0%, respectively. Univariate, multivariate logistic regression, and spatial cluster analyses were performed separately. Sex, age, number of bed nets, forest cover, altitude and household density were potential risk factors. A statistically significant malaria cluster was identified. Significant differences among risk factors were observed between cluster and non-cluster areas.
Malaria has significantly decreased within 2 years after onset of intervention program. Both aspects of the physical and social environment, as well as demographic characteristics are associated with spatial heterogeneity of risk. The ability to identify and locate these areas provides a strategy for targeting interventions during initial stages of intervention programs. However, in high risk clusters of transmission, even extensive coverage by current programs leaves transmission ongoing at reduced levels. This indicates the need for continued development of new strategies for identification and treatment as well as improved understanding of the patterns and determinants of parasitaemia.
疟疾是孟加拉国的一个主要公共卫生问题,在吉大港山区高度流行,2007 年的发病率为 11.7%。一个分区,拉贾斯塔利,发病率为 36%。2007 年初引入了几项干预措施来控制疟疾。本研究旨在评估这些早期强化干预措施对孟加拉国疟疾的影响。这项患病率研究评估高疟疾患病率是否仍然存在,如果存在,哪些地区和人群仍然面临高感染风险。
采用两阶段聚类抽样技术,对拉贾斯塔利的 5322 户家庭中的 1400 户进行抽样,并使用快速诊断测试(Falci-vax)进行筛查。总体疟疾患病率为 11.5%。恶性疟原虫、间日疟原虫和混合感染的比例分别为 93.2%、1.9%和 5.0%。分别进行了单变量、多变量逻辑回归和空间聚类分析。性别、年龄、蚊帐数量、森林覆盖率、海拔和家庭密度是潜在的危险因素。发现了一个有统计学意义的疟疾聚集区。在集群和非集群地区之间观察到危险因素之间存在显著差异。
在干预计划开始后的 2 年内,疟疾的发病率显著下降。物理和社会环境的两个方面以及人口特征都与风险的空间异质性有关。识别和定位这些区域的能力为在干预计划的初始阶段针对干预措施提供了策略。然而,在传播的高风险集群中,即使目前的方案广泛覆盖,传播仍以较低水平持续进行。这表明需要继续开发新的识别和治疗策略,并更好地了解寄生虫血症的模式和决定因素。