Department of Surgery, Leiden University Medical Centre, Leiden, The Netherlands.
Ann Surg Oncol. 2011 Jul;18(7):1821-9. doi: 10.1245/s10434-010-1511-4. Epub 2011 May 5.
Centralization of pancreatic surgery in high-volume hospitals is under debate in many countries. In the western part of the Netherlands, the professional network of surgical oncologists agreed to centralize all pancreatic surgery from 2006 in two high-volume hospitals. Our aim is to evaluate whether centralization of pancreatic surgery has improved clinical outcomes and has changed referral patterns.
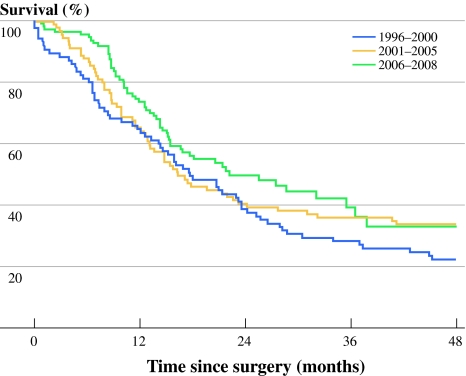
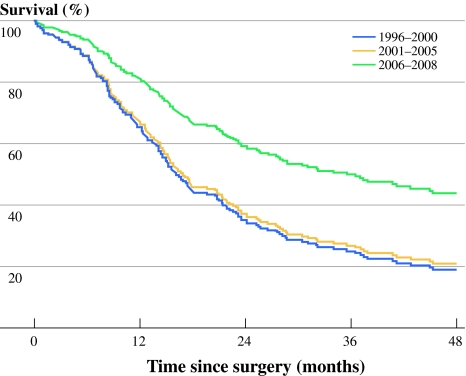
Data of the Comprehensive Cancer Centre West (CCCW) of all 249 patients who had a resection for suspected pancreatic cancer between 1996 and 2008 in the western part of the Netherlands were analyzed. Multivariable modeling was used to evaluate survival for 3 time periods; 1996-2000, 2001-2005 (introduction of quality standards), and 2006-2008 (after centralization). In addition, the differences in referral pattern were analyzed.
From 2006, all pancreatic surgery was centralized in 2 hospitals. The 2-year survival rate increased after centralization from 39% to 55% (P =.09) for all patients who had a pancreatic resection for pancreatic cancer. After adjustment for age, tumor location, stage, histology, and adjuvant treatment, the latter period was significantly associated with improved survival (hazard ratio [HR] 0.50; 95% confidence interval [95% CI] 0.34-0.73).
Centralization of pancreatic surgery was successful and has resulted in improved clinical outcomes in the western part of the Netherlands, demonstrating the effectiveness of centralization.
在许多国家,胰腺手术的集中化在高容量医院中受到争议。在荷兰西部,外科肿瘤学家的专业网络同意自 2006 年起将所有胰腺手术集中在两家高容量医院进行。我们的目的是评估胰腺手术的集中化是否改善了临床结果并改变了转诊模式。
分析了荷兰西部综合癌症中心(CCCW)在 1996 年至 2008 年间所有 249 例疑似胰腺癌患者接受切除术的数据。使用多变量模型评估了 3 个时间段的生存率:1996-2000 年、2001-2005 年(引入质量标准)和 2006-2008 年(集中化后)。此外,还分析了转诊模式的差异。
自 2006 年以来,所有胰腺手术都集中在 2 家医院进行。所有接受胰腺切除术治疗胰腺癌的患者的 2 年生存率在集中化后从 39%提高到 55%(P =.09)。调整年龄、肿瘤位置、分期、组织学和辅助治疗后,后一时期与生存率的提高显著相关(风险比[HR] 0.50;95%置信区间[95%CI] 0.34-0.73)。
胰腺手术的集中化在荷兰西部取得了成功,并导致临床结果的改善,证明了集中化的有效性。