Fischer Claudia, Lingsma Hester, Klazinga Niek, Hardwick Richard, Cromwell David, Steyerberg Ewout, Groene Oliver
Erasmus MC, Department of Public Health, Rotterdam, The Netherlands.
Amsterdam Medical Center, Department of Public Health, Amsterdam, The Netherlands.
PLoS One. 2017 Oct 26;12(10):e0183955. doi: 10.1371/journal.pone.0183955. eCollection 2017.
Most studies showing a volume outcome effect in resection surgery for oesophago-gastric cancer were conducted before the centralisation of clinical services. This study evaluated the relation between hospital- and surgeon volume and different risk-adjusted outcomes after oesophago-gastric (OG) cancer surgery in England between 2011 and 2013.
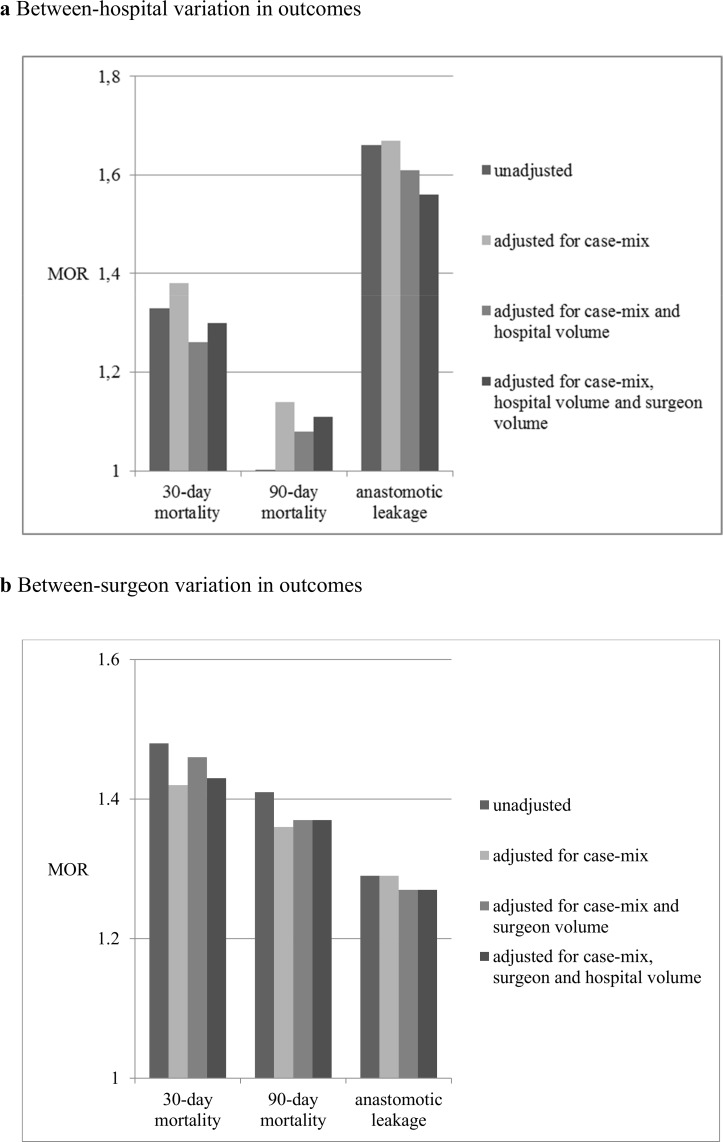
In data from the National Oesophago-Gastric Cancer Audit from the UK, multivariable random-effects logistic regression models were used to quantify the effect of surgeon and hospital volume on three outcomes: 30-day and 90-day mortality and anastomotic leakage. The models included patient risk factors to adjust for differences in case-mix among hospitals and surgeons. The between-cluster heterogeneity was estimated with the median odds ratio (MOR).
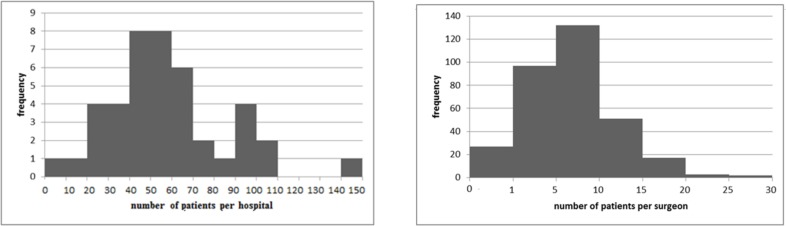
The study included patients treated at 42 hospitals and 329 surgeons. The median (interquartile range) of the annual hospital and surgeon volumes were 110 patients (82 to 137) and 13 patients (8 to 19), respectively. The overall rates for 30-day and 90-day mortality were 2.3% and 4.4% respectively, and the anastomotic leakage was 6.3%. Higher hospital volume was associated with lower 30-day mortality (OR: 0.94; 95% CI: 0.91-0.98) and lower anastomotic leakage rates (OR: 0.96; 95% CI: 0.93-0.98) but not 90-day mortality. Higher surgeon volume was only associated with lower anastomotic leakage rates (OR: 0.81; 95% CI: 0.72-0.92). Hospital volume explained a part of the between-hospital variation in 30-day mortality whereas surgeon volume explained part of the between-hospital variation in anastomotic leakage.
In the setting of centralized O-G cancer surgery in England, we could still observe an effect of volume on short-term outcomes. However, the effect is inconsistent, depending on the type of outcome measure under consideration, and much smaller than in previous studies. Efforts to centralise O-G cancer services further should carefully address the effects of both hospital and surgeon volume on the range of outcome measures that are relevant to patients.
大多数显示食管癌和胃癌切除手术存在容量结局效应的研究是在临床服务集中化之前进行的。本研究评估了2011年至2013年期间英格兰食管癌和胃癌(OG)手术中医院容量、外科医生手术量与不同风险调整结局之间的关系。
在英国国家食管癌和胃癌审计的数据中,使用多变量随机效应逻辑回归模型来量化外科医生手术量和医院容量对三种结局的影响:30天和90天死亡率以及吻合口漏。模型纳入了患者风险因素,以调整医院和外科医生之间病例组合的差异。使用中位数优势比(MOR)估计聚类间异质性。
该研究纳入了在42家医院接受治疗的患者以及329名外科医生。每年医院手术量和外科医生手术量的中位数(四分位间距)分别为110例患者(82至137例)和13例患者(8至19例)。30天和90天死亡率的总体发生率分别为2.3%和4.4%,吻合口漏发生率为6.3%。较高的医院手术量与较低的30天死亡率(比值比:0.94;95%置信区间:0.91 - 0.98)和较低的吻合口漏发生率(比值比:0.96;95%置信区间:0.93 - 0.98)相关,但与90天死亡率无关。较高的外科医生手术量仅与较低的吻合口漏发生率相关(比值比:0.81;95%置信区间:0.72 - 0.92)。医院手术量解释了30天死亡率医院间差异的一部分,而外科医生手术量解释了吻合口漏医院间差异的一部分。
在英格兰食管癌和胃癌手术集中化的背景下,我们仍然可以观察到手术量对短期结局的影响。然而,这种影响并不一致,取决于所考虑的结局指标类型,并且比以往研究中的影响要小得多。进一步集中食管癌和胃癌服务的努力应仔细考虑医院手术量和外科医生手术量对与患者相关的一系列结局指标的影响。