Jonsson Helgi, Helgadottir Gudrun P, Aspelund Thor, Eiriksdottir Gudny, Sigurdsson Sigurdur, Siggeirsdottir Kristin, Ingvarsson Thorvaldur, Harris Tamara B, Launer Lenore, Gudnason Vilmundur
Landspitalinn University Hospital, University of Iceland, Reykjavik, Iceland.
Open Rheumatol J. 2011 Jan 13;5:7-12. doi: 10.2174/1874312901105010007.
To identify factors associated with having total knee replacement due to osteoarthritis in the AGES-Reykjavik Study, a large population based study of elderly Icelanders.
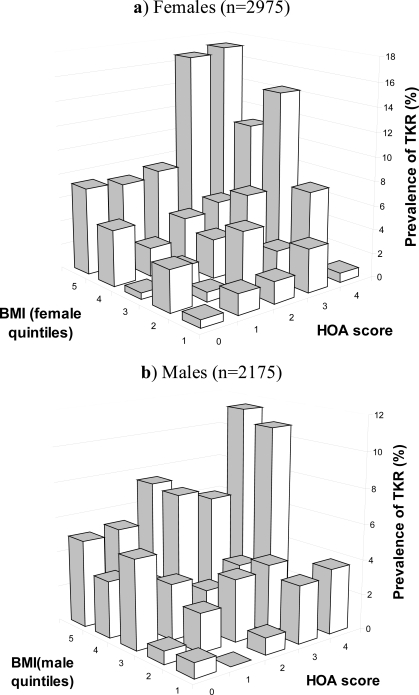
Information about total knee and hip joint replacements (TKR,THR) and hand OA (HOA) severity was available in 2195 males and 2975 females, mean age 76±6 years. The prevalence of TKR was 223 (4.3%) and THR 316 (6.1%). We performed a backwards binary logistic regression analysis of possible OA associated variables including age, gender, abdominal circumference, BMI, hs-CRP, cholesterol, statin use, bone mineral density of the spine, education and smoking history as well as HOA severity and the presence of THR.
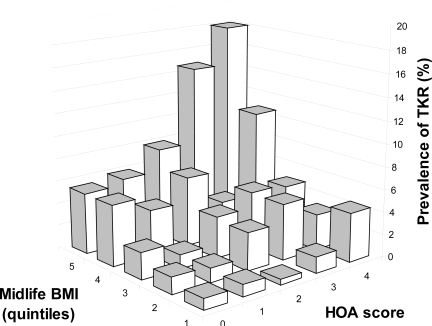
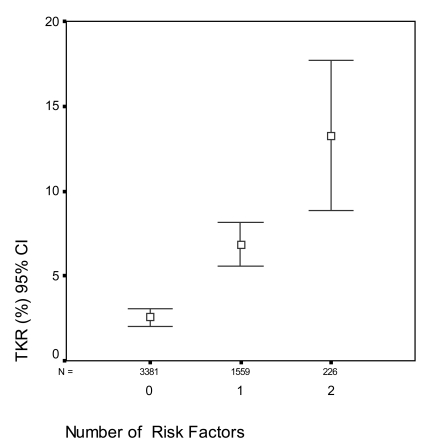
Only three factors showed significant associations with TKR; BMI (p=3.5x10(-17)), HOA severity (p=2.9x10(-8)) and THR (p=0.0002). The highest quintile of BMI was associated with a fivefold risk of TKR compared with the lowest (8% vs 1.6%), and severe HOA had a 2.4 fold risk compared with those with no HOA (8% vs 3.3%). There was no statistical interaction between BMI and HOA. Thus, individuals with BMI<23.5 with no evidence of HOA had a prevalence of TKR of 1.1%, while those with BMI>30.3 and severe HOA had a prevalence of 13.4%.
Hand and hip osteoarthritis in conjunction with BMI are strongly associated with the prevalence of TKR due to osteoarthritis. Together, BMI and HOA severity seem to contribute to the majority of the total TKR prevalence. While BMI has long been recognized as the major risk factor for TKR, the influence of osteoarthritis at other sites may have been underestimated.
在AGES-雷克雅未克研究中确定与因骨关节炎进行全膝关节置换相关的因素,该研究是一项针对冰岛老年人群的大型基于人群的研究。
在2195名男性和2975名女性(平均年龄76±6岁)中可获取有关全膝关节和髋关节置换(TKR、THR)以及手部骨关节炎(HOA)严重程度的信息。TKR的患病率为223例(4.3%),THR为316例(6.1%)。我们对可能与骨关节炎相关的变量进行了向后二元逻辑回归分析,这些变量包括年龄、性别、腹围、BMI、hs-CRP、胆固醇、他汀类药物使用情况、脊柱骨密度、教育程度和吸烟史以及HOA严重程度和THR的存在情况。
只有三个因素与TKR有显著关联;BMI(p = 3.5×10⁻¹⁷)、HOA严重程度(p = 2.9×10⁻⁸)和THR(p = 0.0002)。与最低五分位数相比,BMI最高五分位数的TKR风险高出五倍(8%对1.6%),与无HOA者相比,严重HOA的风险高出2.4倍(8%对3.3%)。BMI和HOA之间无统计学交互作用。因此,BMI<23.5且无HOA证据者的TKR患病率为1.1%,而BMI>30.3且患有严重HOA者的患病率为13.4%。
手部和髋部骨关节炎与BMI共同与因骨关节炎导致的TKR患病率密切相关。BMI和HOA严重程度似乎共同导致了大多数TKR患病率。虽然BMI长期以来一直被认为是TKR的主要危险因素,但其他部位骨关节炎的影响可能被低估了。