Ortega-Andreu Miguel, Pérez-Chrzanowska Hanna, Figueredo Reyes, Gómez-Barrena Enrique
Department of Orthopaedics "A", La Paz Hospital at Cantoblanco, Madrid, Spain.
Open Orthop J. 2011 Mar 16;5:44-8. doi: 10.2174/1874325001105010044.
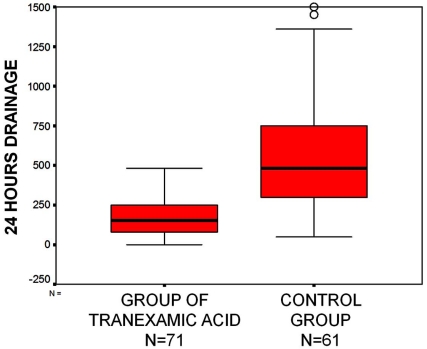
Average blood loss after total knee arthroplasty (TKA) usually ranges from 1500 to 1900 cc, including both the postoperative drain and hidden blood loss. This represents about 46% of TKA patients requiring postoperative blood transfusion. Not only the risks of disease transmission but also those of ABO incompatibility, infection due to immunosupression, increased procedure costs, and increased length of hospital stay, are potential problems that foster blood saving strategies. In this study, 71 unilateral TKAs using a multimodal protocol to decrease blood loss were compared to 61 historical cases. Patients in both groups underwent cemented TKA with the same system, surgical technique, and multimodal protocol (MIS approach, plug in the femoral canal, tourniquet removal after wound closure and compressive bandage, analgesic periarticular infiltration with vasoconstrictor, postoperative drain at atmospheric pressure, opened 2 hours after the end of the surgical procedure and removed after 24 hours). The study series incorporated intravenous tranexamic acid (TXA) infusion in 2 doses of 10-15 mg/kg, 15 minutes before tourniquet release and 3 hours later. Results showed no transfusion requirements in the TXA series (0%), with 23/61 (37.7%) transfusions in the control, with an average cost decrease of 240 euros per patient. Visible bleeding in 24h significantly decreased from 553.36 cc (range 50-1500) to 169.72 cc (range 10-480) in the TXA series. As a conclusion, implementing a TXA-based multimodal protocol produced significant decrease in the transfusion rate, visible blood loss, and cost per patient, thus proving effectiveness and efficiency in the surgical management of TKA.
全膝关节置换术(TKA)后的平均失血量通常在1500至1900毫升之间,包括术后引流液和隐性失血。这意味着约46%的TKA患者需要术后输血。不仅存在疾病传播风险,还有ABO血型不相容、免疫抑制导致的感染、手术成本增加以及住院时间延长等风险,这些都是促使采取血液节约策略的潜在问题。在本研究中,将71例采用多模式方案减少失血的单侧TKA与61例历史病例进行了比较。两组患者均使用相同系统、手术技术和多模式方案(微创入路、股骨管内植入、伤口闭合后松开止血带并使用加压绷带、关节周围浸润麻醉并使用血管收缩剂、术后常压引流、手术结束2小时后打开并在24小时后拔除)进行骨水泥型TKA。研究组在止血带松开前15分钟和3小时后分两次静脉输注氨甲环酸(TXA),剂量为10 - 15毫克/千克。结果显示,TXA组无输血需求(0%),对照组有23/61(37.7%)患者接受输血,每位患者平均成本降低240欧元。TXA组24小时内可见失血量从553.36毫升(范围50 - 1500)显著降至169.72毫升(范围10 - 480)。总之,实施基于TXA的多模式方案可显著降低输血率、可见失血量和每位患者的成本,从而证明其在TKA手术管理中的有效性和高效性。