The Hepatobiliary Division, Department of General Surgery, The First Affiliated Hospital, Wenzhou Medical College, Wenzhou, China.
Cell Biochem Biophys. 2011 Nov;61(2):413-9. doi: 10.1007/s12013-011-9203-7.
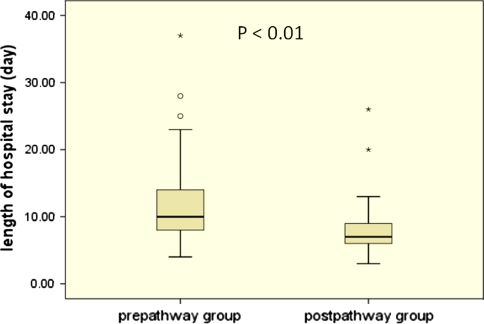
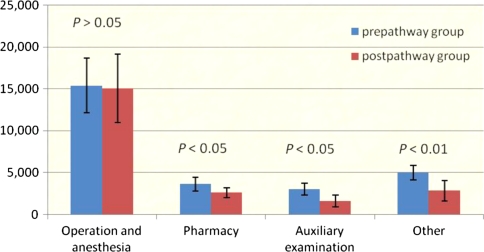
A fast-track clinical pathway is designed to streamline patient care delivery and maximize cost effectiveness. It has decreased postoperative length of stay (LOS) and hospital charges for many surgical procedures. However, data on clinical pathways after liver surgery are sparse. This study examined whether use of a fast-track clinical pathway for patients undergoing elective liver resection affected postoperative LOS and hospital charges. A fast-track clinical pathway was developed and implemented by a multidisciplinary team for patients undergoing liver resection. Between July, 2007 and May, 2008, a total of 117 patients underwent elective liver resection: the fast-track clinical pathway (education of patients and families, earlier oral feeding, earlier discontinuation of intravenous fluid, no drains or nasogastric tubes, early ambulation, use of a urinary catheter for less than 24 h and planned discharge 6 days after surgery) was studied prospectively in 56 patients (postpathway group). These patients were compared with the remainder who had usual care (prepathway group). Outcome measures were postoperative LOS, perioperative hospital charges, intraoperative and postoperative complications, mortality, and readmission rate. Among all patients, 69 (59%) had complicating diseases and/or a history of surgery and 24 patients belonged to American Society of Anesthesiologists grade III-IV. Compared with the prepathway group, the postpathway group had a significantly shorter postoperative LOS (7 vs. 11 days, P < 0.01). The average perioperative hospital charges were RMB 26,626 for patients in the prepathway group and only RMB 21,004 for those in the postpathway group (P < 0.05), with no differences in intraoperative and postoperative complications (P = 0.814), mortality (P = 0.606), and readmission rate (P = 0.424). Implementation of the fast-track clinical pathway is an effective and safe method for reducing postoperative LOS and hospital charges for high-risk patients undergoing elective liver resection. The result supports the further development of fast-track clinical pathways for liver surgical procedures.
快速通道临床路径旨在简化患者护理流程并实现成本效益最大化。它已缩短了许多外科手术的术后住院时间(LOS)和住院费用。然而,关于肝手术后临床路径的数据很少。本研究探讨了接受择期肝切除术的患者使用快速通道临床路径是否会影响术后 LOS 和住院费用。一个多学科团队为接受肝切除术的患者制定并实施了快速通道临床路径。2007 年 7 月至 2008 年 5 月,共有 117 例患者接受择期肝切除术:前瞻性研究了 56 例患者(路径后组)接受快速通道临床路径(患者和家属教育、早期口服喂养、提前停止静脉输液、无引流管或鼻胃管、早期活动、使用导尿管少于 24 小时和计划术后 6 天出院)。这些患者与接受常规护理的其余患者(路径前组)进行比较。观察指标为术后 LOS、围手术期住院费用、术中及术后并发症、死亡率和再入院率。所有患者中,69 例(59%)有合并症和/或手术史,24 例患者属于美国麻醉医师协会(ASA)分级 III-IV 级。与路径前组相比,路径后组的术后 LOS 明显缩短(7 天比 11 天,P <0.01)。路径前组患者的平均围手术期住院费用为 26626 元,路径后组仅为 21004 元(P <0.05),但术中及术后并发症无差异(P =0.814),死亡率(P =0.606)和再入院率(P =0.424)。对于接受择期肝切除术的高危患者,实施快速通道临床路径是一种有效且安全的方法,可缩短术后 LOS 和住院费用。结果支持进一步开发肝外科手术的快速通道临床路径。