St James's University Hospital and University of Leeds, Leeds, UK.
Lancet. 2011 May 21;377(9779):1749-59. doi: 10.1016/S0140-6736(11)60399-1. Epub 2011 May 11.
Elderly and frail patients with cancer, although often treated with chemotherapy, are under-represented in clinical trials. We designed FOCUS2 to investigate reduced-dose chemotherapy options and to seek objective predictors of outcome in frail patients with advanced colorectal cancer.
We undertook an open, 2 × 2 factorial trial in 61 UK centres for patients with previously untreated advanced colorectal cancer who were considered unfit for full-dose chemotherapy. After comprehensive health assessment (CHA), patients were randomly assigned by minimisation to: 48-h intravenous fluorouracil with levofolinate (group A); oxaliplatin and fluorouracil (group B); capecitabine (group C); or oxaliplatin and capecitabine (group D). Treatment allocation was not masked. Starting doses were 80% of standard doses, with discretionary escalation to full dose after 6 weeks. The two primary outcome measures were: addition of oxaliplatin ([A vs B] + [C vs D]), assessed with progression-free survival (PFS); and substitution of fluorouracil with capecitabine ([A vs C] + [B vs D]), assessed by change from baseline to 12 weeks in global quality of life (QoL). Analysis was by intention to treat. Baseline clinical and CHA data were modelled against outcomes with a novel composite measure, overall treatment utility (OTU). This study is registered, number ISRCTN21221452.
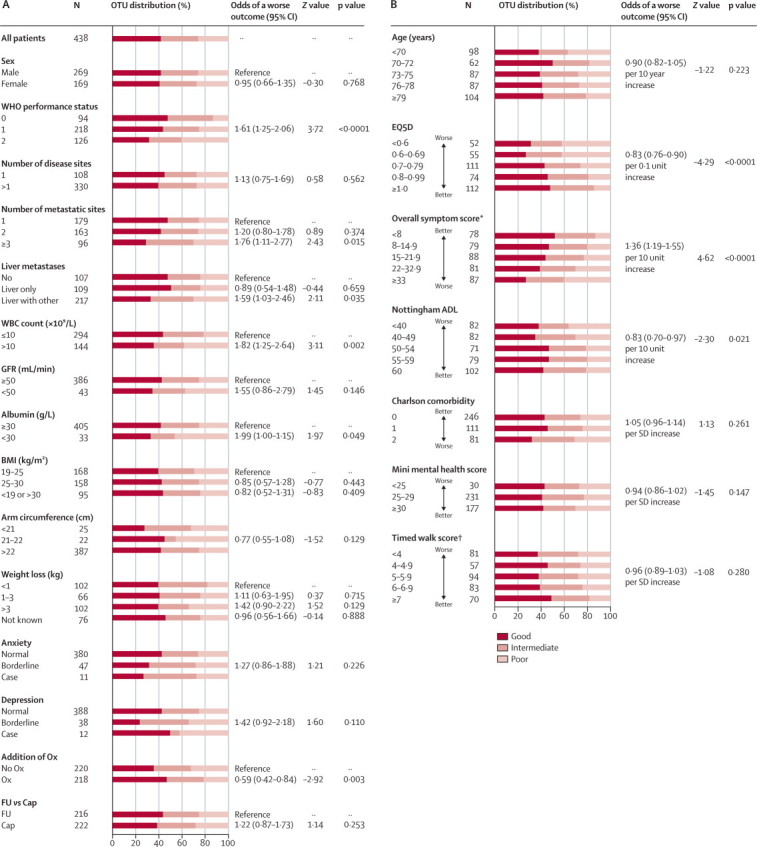
459 patients were randomly assigned (115 to each of groups A-C, 114 to group D). Factorial comparison of addition of oxaliplatin versus no addition suggested some improvement in PFS, but the finding was not significant (median 5·8 months [IQR 3·3-7·5] vs 4·5 months [2·8-6·4]; hazard ratio 0·84, 95% CI 0·69-1·01, p=0·07). Replacement of fluorouracil with capecitabine did not improve global QoL: 69 of 124 (56%) patients receiving fluorouracil reported improvement in global QoL compared with 69 of 123 (56%) receiving capecitabine. The risk of having any grade 3 or worse toxic effect was not significantly increased with oxaliplatin (83/219 [38%] vs 70/221 [32%]; p=0·17), but was higher with capecitabine than with fluorouracil (88/222 [40%] vs 65/218 [30%]; p=0·03). In multivariable analysis, fewer baseline symptoms (odds ratio 1·32, 95% CI 1·14-1·52), less widespread disease (1·51, 1·05-2·19), and use of oxaliplatin (0·57, 0·39-0·82) were predictive of better OTU.
FOCUS2 shows that with an appropriate design, including reduced starting doses of chemotherapy, frail and elderly patients can participate in a randomised controlled trial. On balance, a combination including oxaliplatin was preferable to single-agent fluoropyrimidines, although the primary endpoint of PFS was not met. Capecitabine did not improve QoL compared with fluorouracil. Comprehensive baseline assessment holds promise as an objective predictor of treatment benefit.
Cancer Research UK and the Medical Research Council.

患有癌症的老年和体弱患者,尽管经常接受化疗治疗,但在临床试验中的代表性不足。我们设计了 FOCUS2,旨在研究低剂量化疗方案,并寻找晚期结直肠癌虚弱患者预后的客观预测因素。
我们在英国 61 个中心开展了一项开放性、2×2 析因试验,纳入了先前未经治疗的晚期结直肠癌且认为不能耐受全剂量化疗的患者。在全面健康评估(CHA)后,患者通过最小化法随机分配至:48 小时静脉注射氟尿嘧啶+左亚叶酸(A 组);奥沙利铂+氟尿嘧啶(B 组);卡培他滨(C 组);或奥沙利铂+卡培他滨(D 组)。治疗分配未设盲。起始剂量为标准剂量的 80%,6 周后可自由调整至全剂量。主要终点为:奥沙利铂的添加(A 与 B 的比较,C 与 D 的比较),用无进展生存期(PFS)评估;氟尿嘧啶被卡培他滨替代(A 与 C 的比较,B 与 D 的比较),用 12 周时全球生活质量(QoL)相对于基线的变化来评估。分析采用意向治疗。基于基线临床和 CHA 数据,采用一种新的综合治疗效果测量方法(OTU)进行结果建模。本研究已注册,编号为 ISRCTN21221452。
459 名患者被随机分配(每组 A-C 115 例,D 组 114 例)。奥沙利铂添加与不添加的析因比较提示 PFS 略有改善,但无统计学意义(中位数 5.8 个月[IQR 3.3-7.5]比 4.5 个月[2.8-6.4];风险比 0.84,95%CI 0.69-1.01,p=0.07)。氟尿嘧啶被卡培他滨替代并没有改善全球 QoL:接受氟尿嘧啶治疗的 124 名患者中有 69 名(56%)报告全球 QoL 改善,而接受卡培他滨治疗的 123 名患者中有 69 名(56%)报告全球 QoL 改善。奥沙利铂治疗的 3 级或更高级别毒性反应风险没有显著增加(83/219 [38%]比 70/221 [32%];p=0.17),但卡培他滨的风险高于氟尿嘧啶(88/222 [40%]比 65/218 [30%];p=0.03)。多变量分析显示,基线症状较少(比值比 1.32,95%CI 1.14-1.52)、疾病广泛程度较低(比值比 1.51,95%CI 1.05-2.19)和使用奥沙利铂(比值比 0.57,95%CI 0.39-0.82)是治疗效果更好的 OTU 的预测因素。
FOCUS2 表明,通过适当的设计,包括降低化疗的起始剂量,体弱和老年患者可以参与随机对照试验。总的来说,包括奥沙利铂的联合治疗比单药氟嘧啶更有优势,尽管主要终点 PFS 未达到。卡培他滨与氟尿嘧啶相比并没有改善 QoL。全面的基线评估有望成为治疗获益的客观预测因素。
英国癌症研究中心和医学研究委员会。