Diercks Deborah B, Kirk J Douglas, Naser Seif, Turnipseed Samuel, Amsterdam Ezra A
Department of Emergency Medicine, University of California, Davis Medical Center, Sacramento, CA, USA.
Int J Emerg Med. 2011 Jun 24;4:37. doi: 10.1186/1865-1380-4-37.
High-sensitivity C-reactive protein (hs-CRP) rises with cardiac injury/ischemia. We evaluated its efficacy in aiding in the identification of an acute coronary syndrome (ACS) in patients (pts) admitted to the chest pain unit (CPU) for possible ACS.
Retrospective study of all patients admitted to the CPU with chest pain who underwent hs-CRP testing as part of their CPU evaluation from January 2004 to October 2008. Patients were low risk for ACS (compatible symptoms, nondiagnostic initial ECG, and negative cTnI). ACS was diagnosed by positive functional study, cardiac catheterization, or cardiac event during 30-day follow-up. Positive hs-CRP was defined based on local laboratory levels (>1.0 mg/l or >3.0 mg/l), and population-based and prior study values >2.0 mg/l. Chi-square analysis was performed, and odds ratios (OR) are presented. Multivariate analysis was done to determine whether hs-CRP was independently associated with the diagnosis of ACS. Cardiac risk factors, demographics, and diagnosis of ACS were included in the model. Medians with IQR are presented for continuous data. Ninety-five percent confidence intervals are presented where applicable.
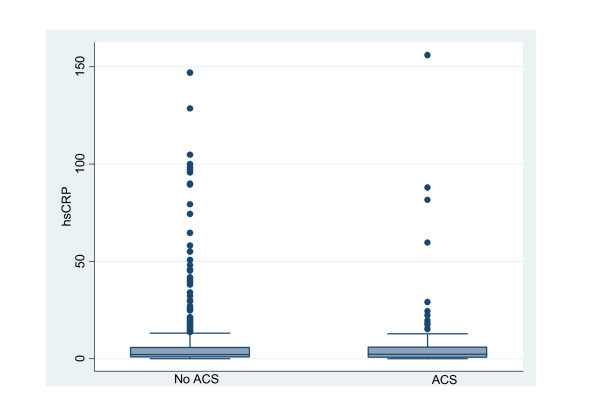
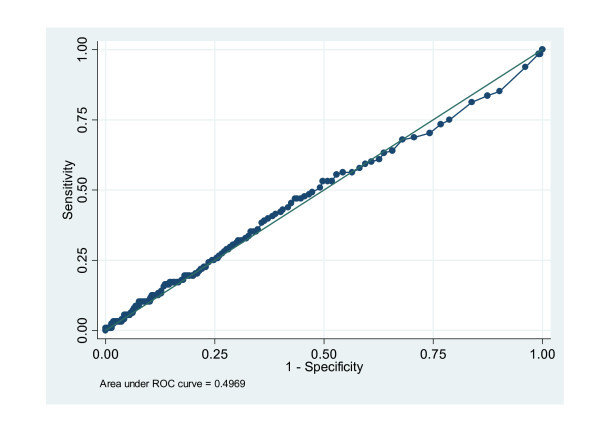
A total of 958 patients had hs-CRP testing as part of their CPEU evaluation. Excluded from the analysis were 39 patients lost to follow-up. The final cohort comprised 478 (52%) women and 441 (48%) men with a median age of 56 (IQR 48-64). ACS was diagnosed in 128 (13.4%). The median cohort hs-CRP value was 2.2 mg/l (IQR 0.7, 5.8) and 2.3 mg/l (IQR 0.6, 5.9) in those with and without ACS, respectively. In the multivariate analysis hs-CRP was not independently associated with the diagnosis of ACS (0.99; 95% CI 0.98 - 1.01).
In large patient cohort managed in a single-center CPU, measurement of hs-CRP did not enhance the diagnostic accuracy for ACS. Routine hs-CRP as a diagnostic tool should not be recommended in the CPU setting.
高敏C反应蛋白(hs-CRP)水平会随心脏损伤/缺血而升高。我们评估了其在协助诊断因可能患有急性冠状动脉综合征(ACS)而入住胸痛单元(CPU)的患者(pts)中的作用。
对2004年1月至2008年10月期间因胸痛入住CPU且接受hs-CRP检测作为其CPU评估一部分的所有患者进行回顾性研究。这些患者为ACS低风险患者(症状相符、初始心电图无诊断意义且肌钙蛋白I阴性)。通过功能检查阳性、心脏导管检查或30天随访期间发生心脏事件来诊断ACS。根据当地实验室水平(>1.0 mg/l或>3.0 mg/l)以及基于人群和先前研究的值>2.0 mg/l来定义hs-CRP阳性。进行卡方分析并给出比值比(OR)。进行多变量分析以确定hs-CRP是否与ACS诊断独立相关。模型中纳入了心脏危险因素、人口统计学特征和ACS诊断。对于连续数据给出中位数及四分位间距(IQR)。在适用的情况下给出95%置信区间。
共有958例患者接受了hs-CRP检测作为其CPEU评估的一部分。分析中排除了39例失访患者。最终队列包括478名(52%)女性和441名(48%)男性,中位年龄为56岁(IQR 48 - 64)。128例(13.4%)患者被诊断为ACS。有ACS和无ACS患者队列的hs-CRP中位数分别为2.2 mg/l(IQR 0.7, 5.8)和2.3 mg/l(IQR 0.6, 5.9)。在多变量分析中,hs-CRP与ACS诊断无独立相关性(0.99;95% CI 0.98 - 1.01)。
在单中心CPU管理的大型患者队列中,hs-CRP检测并未提高ACS的诊断准确性。在CPU环境中不应推荐将常规hs-CRP作为诊断工具。