Department of Infectious Diseases, St. Jude Children's Research Hospital, Memphis, Tennessee, United States of America.
PLoS Pathog. 2011 Jul;7(7):e1002134. doi: 10.1371/journal.ppat.1002134. Epub 2011 Jul 7.
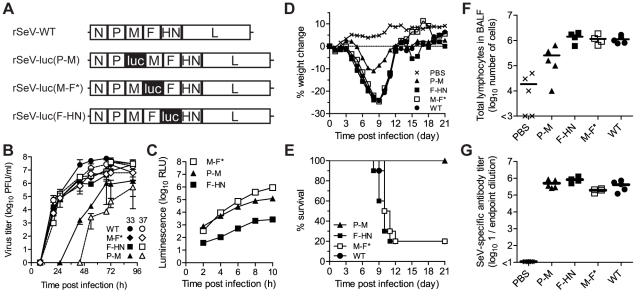
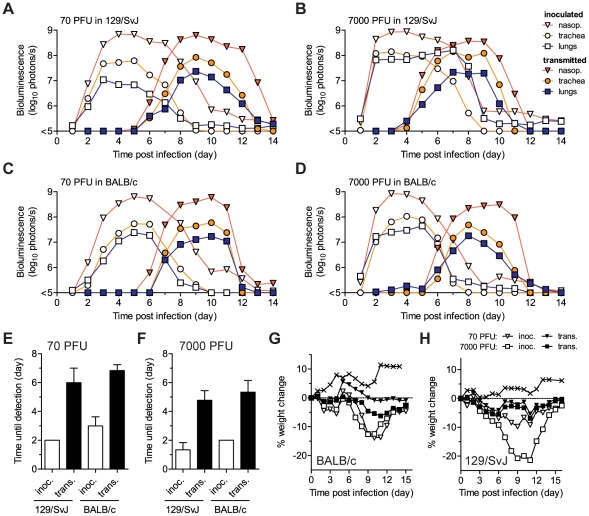
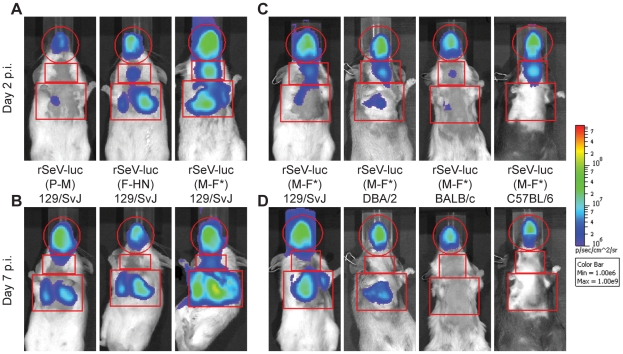
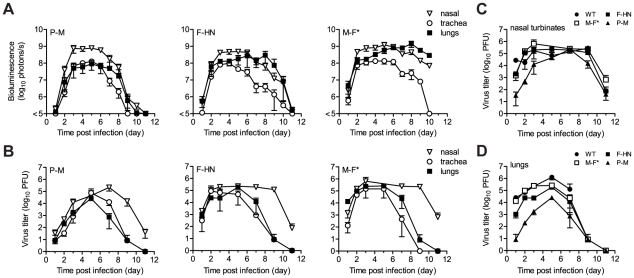
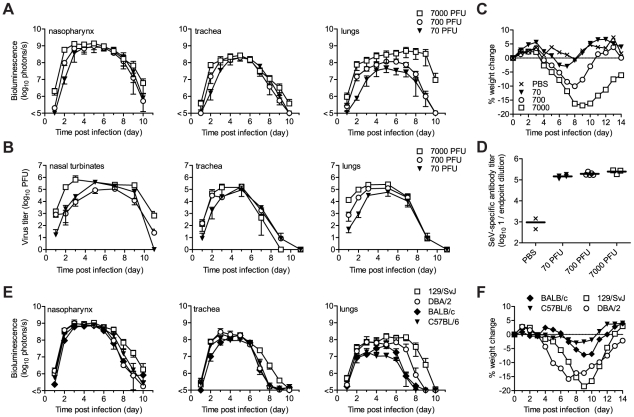
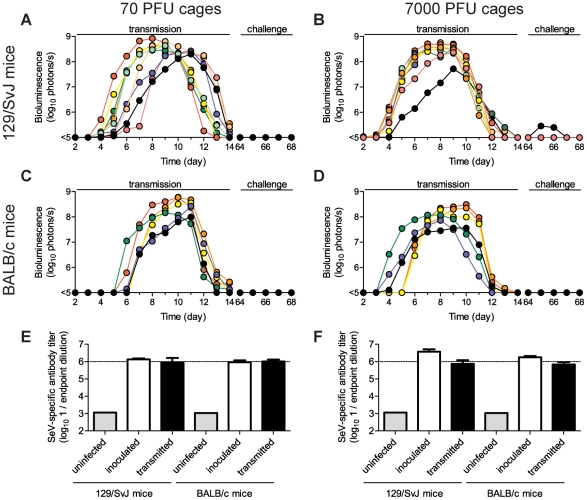
The parainfluenza viruses (PIVs) are highly contagious respiratory paramyxoviruses and a leading cause of lower respiratory tract (LRT) disease. Since no vaccines or antivirals exist, non-pharmaceutical interventions are the only means of control for these pathogens. Here we used bioluminescence imaging to visualize the spatial and temporal progression of murine PIV1 (Sendai virus) infection in living mice after intranasal inoculation or exposure by contact. A non-attenuated luciferase reporter virus (rSeV-luc(M-F*)) that expressed high levels of luciferase yet was phenotypically similar to wild-type Sendai virus in vitro and in vivo was generated to allow visualization. After direct intranasal inoculation, we unexpectedly observed that the upper respiratory tract (URT) and trachea supported robust infection under conditions that result in little infection or pathology in the lungs including a low inoculum of virus, an attenuated virus, and strains of mice genetically resistant to lung infection. The high permissivity of the URT and trachea to infection resulted in 100% transmission to naïve contact recipients, even after low-dose (70 PFU) inoculation of genetically resistant BALB/c donor mice. The timing of transmission was consistent with the timing of high viral titers in the URT and trachea of donor animals but was independent of the levels of infection in the lungs of donors. The data therefore reveals a disconnect between transmissibility, which is associated with infection in the URT, and pathogenesis, which arises from infection in the lungs and the immune response. Natural infection after transmission was universally robust in the URT and trachea yet limited in the lungs, inducing protective immunity without weight loss even in genetically susceptible 129/SvJ mice. Overall, these results reveal a dichotomy between PIV infection in the URT and trachea versus the lungs and define a new model for studies of pathogenesis, development of live virus vaccines, and testing of antiviral therapies.
副黏病毒(PIVs)是高度传染性的呼吸道副黏液病毒,是下呼吸道(LRT)疾病的主要病因。由于没有疫苗或抗病毒药物,因此这些病原体的唯一控制手段是非药物干预。在这里,我们使用生物发光成像技术来可视化活鼠体内鼻内接种或接触感染后鼠副流感病毒 1(仙台病毒)的空间和时间进展。我们生成了一种非衰减的荧光素酶报告病毒(rSeV-luc(M-F*)),该病毒在体外和体内表达高水平的荧光素酶,但表型与野生型仙台病毒相似,从而可以进行可视化。直接鼻内接种后,我们出人意料地观察到上呼吸道(URT)和气管在以下情况下支持强大的感染:在肺部中导致很少感染或病理学的情况下,包括病毒接种量低、病毒衰减和对肺部感染具有遗传抗性的小鼠株。URT 和气管对感染的高度易感性导致 100%的未感染接触受体传播,即使在对肺部感染具有遗传抗性的 BALB/c 供体小鼠进行低剂量(70 PFU)接种时也是如此。传播的时间与供体动物 URT 和气管中高病毒滴度的时间一致,但与供体肺部感染水平无关。因此,数据揭示了传染性与 URT 感染之间的脱节,而发病机制则与肺部感染和免疫反应有关。传播后的自然感染在 URT 和气管中普遍强大,但在肺部中却受到限制,即使在遗传易感的 129/SvJ 小鼠中,也会引起无体重减轻的保护性免疫。总体而言,这些结果揭示了 URT 和气管中的 PIV 感染与肺部之间的二分法,并定义了用于发病机制研究、活病毒疫苗开发和抗病毒疗法测试的新模型。