Institute for Health Service Research, Peninsula College of Medicine and Dentistry, University of Exeter, Exeter, UK.
Int J Behav Nutr Phys Act. 2011 Jul 13;8:73. doi: 10.1186/1479-5868-8-73.
Only limited data are available on the development and feasibility piloting of school-based interventions to prevent and reduce obesity in children. Clear documentation of the rationale, process of development and content of such interventions is essential to enable other researchers to understand why interventions succeed or fail.
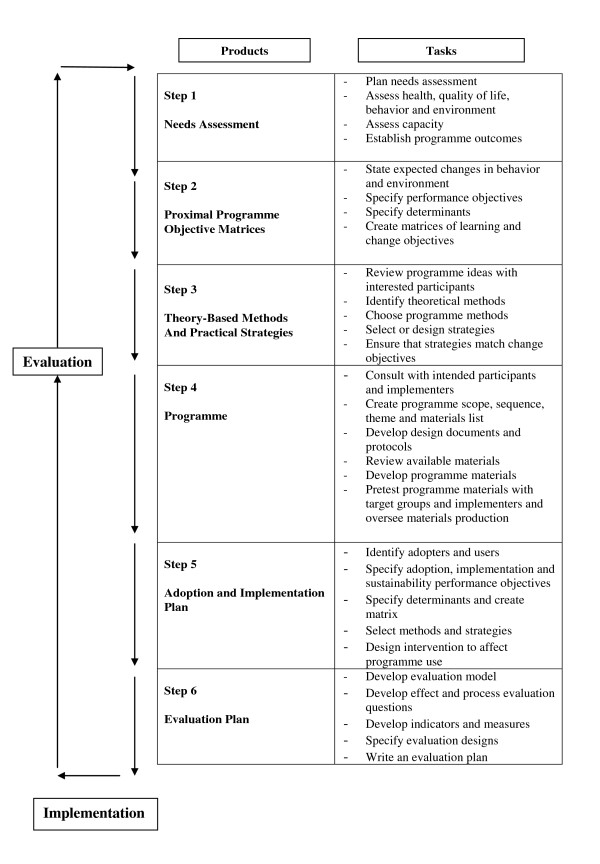
This paper describes the development of the Healthy Lifestyles Programme (HeLP), a school-based intervention to prevent obesity in children, through the first 4 steps of the Intervention Mapping protocol (IM). The intervention focuses on the following health behaviours, i) reduction of the consumption of sweetened fizzy drinks, ii) increase in the proportion of healthy snacks consumed and iii) reduction of TV viewing and other screen-based activities, within the context of a wider attempt to improve diet and increase physical activity.
Two phases of pilot work demonstrated that the intervention was acceptable and feasible for schools, children and their families and suggested areas for further refinement. Feedback from the first pilot phase suggested that the 9-10 year olds were both receptive to the messages and more able and willing to translate them into possible behaviour changes than older or younger children and engaged their families to the greatest extent. Performance objectives were mapped onto 3 three broad domains of behaviour change objectives--establish motivation, take action and stay motivated--in order to create an intervention that supports and enables behaviour change. Activities include whole school assemblies, parents evenings, sport/dance workshops, classroom based education lessons, interactive drama workshops and goal setting and runs over three school terms.
The Intervention Mapping protocol was a useful tool in developing a feasible, theory based intervention aimed at motivating children and their families to make small sustainable changes to their eating and activity behaviours. Although the process was time consuming, this systematic approach ensures that the behaviour change techniques and delivery methods link directly to the Programme's performance objectives and their associated determinants. This in turn provides a clear framework for process analysis and increases the potential of the intervention to realise the desired outcome of preventing and reducing obesity in children.
仅有有限的数据可用于开发和试点基于学校的干预措施,以预防和减少儿童肥胖。明确记录此类干预措施的基本原理、开发过程和内容对于使其他研究人员能够理解干预措施为何成功或失败至关重要。
本文描述了通过干预映射协议(IM)的前 4 个步骤开发基于学校的预防儿童肥胖的干预措施——健康生活方式计划(HeLP)。该干预措施侧重于以下健康行为:i)减少含糖碳酸饮料的消费,ii)增加健康零食的消费比例,iii)减少看电视和其他基于屏幕的活动,同时努力改善饮食和增加体育活动。
两轮试点工作表明,该干预措施对学校、儿童及其家庭是可接受且可行的,并提出了进一步改进的领域。来自第一阶段试点的反馈表明,9-10 岁的儿童既容易接受这些信息,又更有能力和意愿将其转化为可能的行为改变,而年龄较大或较小的儿童则不然,并且他们最大程度地让其家庭参与进来。绩效目标被映射到行为改变目标的三个广泛领域——建立动机、采取行动和保持动机——以创建支持和促进行为改变的干预措施。活动包括全校集会、家长之夜、体育/舞蹈工作坊、课堂教育课程、互动戏剧工作坊以及目标设定和运行三个学期。
干预映射协议是开发基于理论的可行干预措施的有用工具,旨在激励儿童及其家庭对其饮食和活动行为进行微小而可持续的改变。虽然这个过程很耗时,但这种系统的方法确保了行为改变技术和交付方法直接与计划的绩效目标及其相关决定因素相关联。这反过来又为过程分析提供了一个清晰的框架,并增加了干预措施实现预防和减少儿童肥胖的预期结果的潜力。