Department of Anesthesia, Critical Care and Pain Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, USA.
Crit Care Med. 2011 Dec;39(12):2659-64. doi: 10.1097/CCM.0b013e3182281f1b.
Acute kidney injury affects 5% to 7% of all hospitalized patients with a much higher incidence in the critically ill. The Acute Kidney Injury Network proposed a definition in which serum creatinine rises (>0.3 mg/dL) and/or oliguria (<0.5 mL/kg/hr) for a period of 6 hrs are used to detect acute kidney injury. Accurate urine output measurements as well as serum creatinine values from our database were used to detect patients with acute kidney injury and calculate their corresponding mortality risk and length of stay.
Retrospective cohort study.
Seven intensive care units at a large, academic, tertiary medical center.
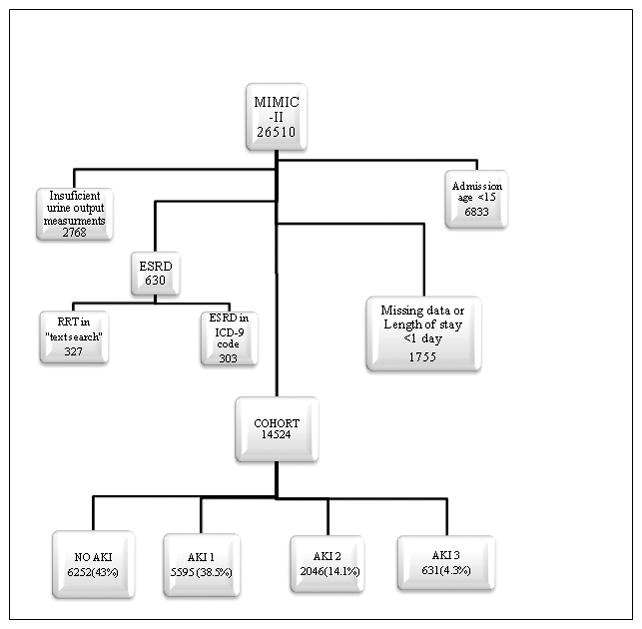
Adult patients without evidence of end-stage renal disease with more than two creatinine measurements and at least a 6-hr urine output recording who were admitted to the intensive care unit between 2001 and 2007.
Medical records of all the patients were reviewed. Demographic information, laboratory results, charted data, discharge diagnoses, physiological data, and patient outcomes were extracted from the Multiparameter Intelligent Monitoring in Intensive Care II database using a SQL query.
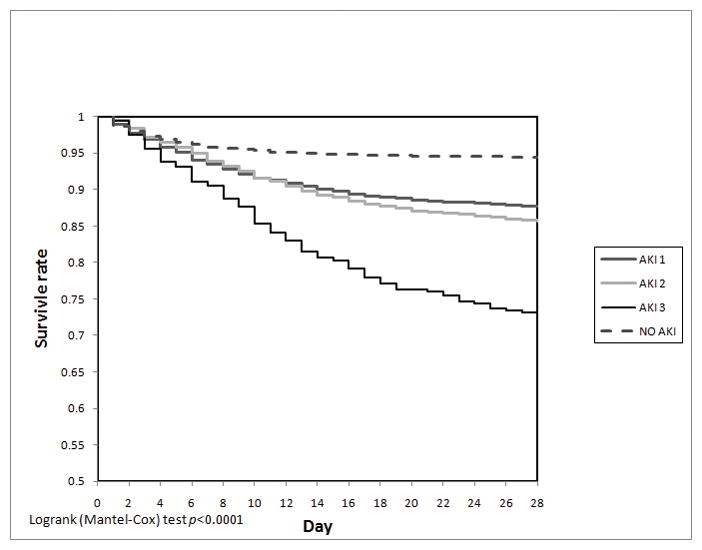
From 19,677 adult patient records, 14,524 patients met the inclusion criteria. Fifty-seven percent developed acute kidney injury during their intensive care unit stay. Inhospital mortality rates were: 13.9%, 16.4%, 33.8% for acute kidney injury 1, 2, and 3, respectively, compared with only 6.2% in patients without acute kidney injury (p < .0001). After adjusting for multiple covariates, acute kidney injury was associated with increased hospital mortality (odds ratio 1.4 and 1.3 for acute kidney injury 1 and acute kidney injury 2 and 2.5 for acute kidney injury 3; p < .0001). Using multivariate logistic regression, we found that in patients who developed acute kidney injury, urine output alone was a better mortality predictor than creatinine alone or the combination of both.
More than 50% of our critically ill patients developed some stage of acute kidney injury resulting in a stagewise increased mortality risk. However, the mortality risk associated with acute kidney injury stages 1 and 2 does not differ significantly. In light of these findings, re-evaluation of the Acute Kidney Injury Network staging criteria should be considered.
急性肾损伤影响所有住院患者的 5%至 7%,而危重症患者的发病率更高。急性肾损伤网络提出了一个定义,即血清肌酐升高(>0.3mg/dL)和/或少尿(<0.5ml/kg/hr)持续 6 小时,用于检测急性肾损伤。我们的数据库中使用准确的尿量测量值和血清肌酐值来检测急性肾损伤患者,并计算其相应的死亡率风险和住院时间。
回顾性队列研究。
一家大型学术性三级医疗中心的七个重症监护病房。
无终末期肾病证据的成年患者,有两次以上的肌酐测量值和至少 6 小时的尿量记录,于 2001 年至 2007 年期间入住重症监护病房。
回顾所有患者的病历。使用 SQL 查询从 Multiparameter Intelligent Monitoring in Intensive Care II 数据库中提取人口统计学信息、实验室结果、图表数据、出院诊断、生理数据和患者结局。
从 19677 份成年患者记录中,有 14524 名患者符合纳入标准。57%的患者在重症监护病房期间发生急性肾损伤。院内死亡率分别为:急性肾损伤 1 期、2 期和 3 期为 13.9%、16.4%和 33.8%,而无急性肾损伤的患者仅为 6.2%(p<0.0001)。在调整了多个协变量后,急性肾损伤与住院死亡率增加相关(急性肾损伤 1 期和 2 期的比值比分别为 1.4 和 1.3,急性肾损伤 3 期为 2.5;p<0.0001)。使用多变量逻辑回归,我们发现在发生急性肾损伤的患者中,尿量单独是死亡率的更好预测指标,优于肌酐单独或两者的组合。
我们的危重症患者中超过 50%发生了某种程度的急性肾损伤,导致死亡率呈阶段性增加。然而,急性肾损伤 1 期和 2 期的死亡率风险没有显著差异。鉴于这些发现,应考虑重新评估急性肾损伤网络分期标准。