AP-HP, Groupe Henri-Mondor Albert-Chenevier, Service de Reanimation Medicale, 51 avenue du Mal de Lattre de Tassigny Creteil, F-94010 France.
Crit Care. 2011 Jul 18;15(4):R171. doi: 10.1186/cc10317.
Recent publications suggest potential benefits from statins as a preventive or adjuvant therapy in sepsis. Whether ongoing statin therapy should be continued or discontinued in patients admitted in the intensive care unit (ICU) for sepsis is open to question.
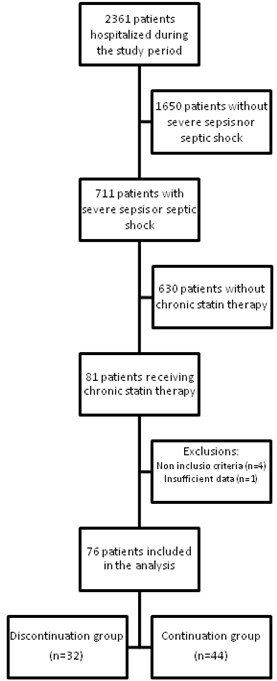
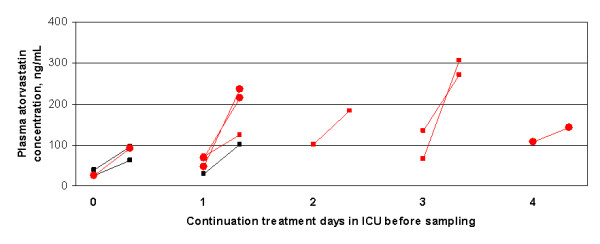
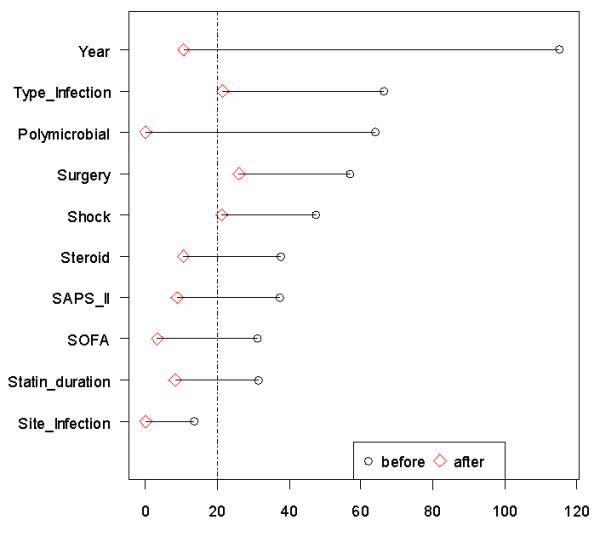
We retrospectively compared patients with severe sepsis and septic shock in whom statin therapy had been discontinued or continued. The primary endpoint was the number of organ failure-free days at day 14. Secondary end-points included hospital mortality and safety. The association of statin continuation with outcome was evaluated for crude analysis and after propensity score matching and adjustment. We also measured plasma atorvastatin concentrations in a separate set of ICU septic patients continuing the drug.
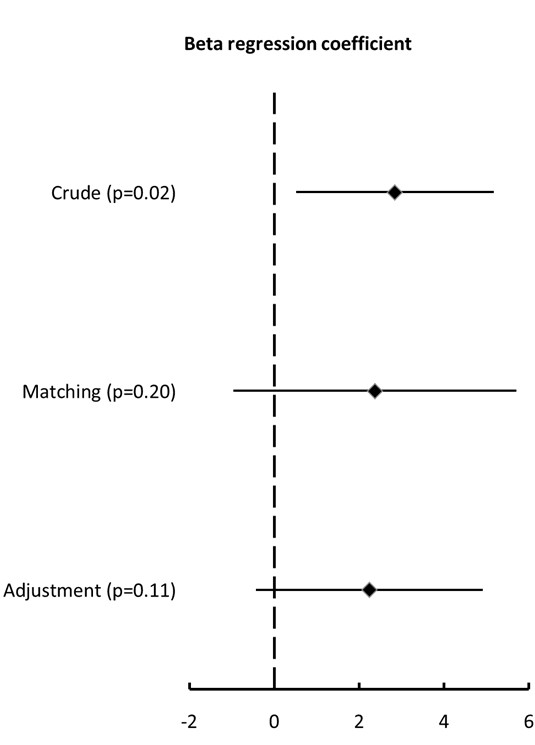
Patients in whom statin therapy had been continued in the ICU (n = 44) had significantly more organ failure-free days (11 67891011121314 vs. 6 [0-12], mean difference of 2.34, 95%CI from 0.47 to 5.21, P = 0.03) as compared to others (n = 32). However, there were important imbalances between groups, with more hospital-acquired infections, more need for surgery before ICU admission, and a trend towards more septic shock at ICU admission in the discontinuation group. The significant association of statin continuation with organ failure free days found in the crude analysis did not persist after propensity-matching or multivariable adjustment: beta coefficients [95% CI] of 2.37 [-0.96 to 5.70] (P = 0.20) and 2.24 [-0.43 to 4.91] (P = 0.11) respectively. We found particularly high pre-dose and post-dose atorvastatin concentrations in ICU septic patients continuing the drug.
Continuing statin therapy in ICU septic patients was not associated with reduction in the severity of organ failure after matching and adjustment. In addition, the very high plasma concentrations achieved during continuation of statin treatment advocates some caution.
最近的出版物表明,他汀类药物作为脓毒症的预防或辅助治疗可能具有潜在益处。对于因脓毒症入住重症监护病房(ICU)的患者,正在进行的他汀类药物治疗是继续还是停止,这是一个悬而未决的问题。
我们回顾性比较了 ICU 中停止或继续他汀类药物治疗的严重脓毒症和感染性休克患者。主要终点是第 14 天无器官衰竭的天数。次要终点包括住院死亡率和安全性。在未校正和校正后倾向评分匹配分析中,评估他汀类药物继续使用与结局的关系。我们还在一组继续使用该药物的 ICU 脓毒症患者中测量了血浆阿托伐他汀浓度。
与其他患者(n = 32)相比,ICU 中继续他汀类药物治疗的患者(n = 44)无器官衰竭天数明显更多(11 67891011121314 天[0-12],平均差异为 2.34,95%CI 为 0.47 至 5.21,P = 0.03)。然而,两组之间存在重要的不平衡,在停药组中,医院获得性感染更多,在 ICU 入院前更需要手术,且 ICU 入院时感染性休克的趋势更为明显。在未校正分析中发现的他汀类药物继续使用与无器官衰竭天数之间的显著相关性在倾向评分匹配或多变量调整后并未持续存在:β系数[95%CI]分别为 2.37[-0.96 至 5.70](P = 0.20)和 2.24[-0.43 至 4.91](P = 0.11)。我们发现继续使用他汀类药物治疗的 ICU 脓毒症患者的阿托伐他汀治疗前和治疗后浓度特别高。
在匹配和调整后,ICU 脓毒症患者继续他汀类药物治疗与器官衰竭严重程度的降低无关。此外,在继续使用他汀类药物治疗期间达到的非常高的血浆浓度需要谨慎。