Toronto Rehabilitation Institute, Toronto, ON, Canada.
Osteoporos Int. 2012 Jan;23(1):87-95. doi: 10.1007/s00198-011-1726-7. Epub 2011 Jul 16.
We conducted a cluster randomized trial evaluating the effect of a centralized coordinator who identifies and follows up with fracture patients and their primary care physicians about osteoporosis. Compared with controls, intervention patients were five times more likely to receive BMD testing and two times more likely to receive appropriate management.
To determine if a centralized coordinator who follows up with fracture patients and their primary care physicians by telephone and mail (intervention) will increase the proportion of patients who receive appropriate post-fracture osteoporosis management, compared to simple fall prevention advice (attention control).
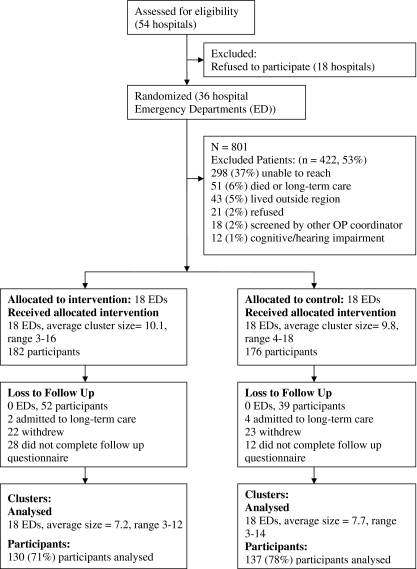
A cluster randomized controlled trial was conducted in small community hospitals in the province of Ontario, Canada. Hospitals that treated between 60 and 340 fracture patients per year were eligible. Patients 40 years and older presenting with a low trauma fracture were identified from Emergency Department records and enrolled in the trial. The primary outcome was 'appropriate' management, defined as a normal bone mineral density (BMD) test or taking osteoporosis medications.
Thirty-six hospitals were randomized to either intervention or control and 130 intervention and 137 control subjects completed the study. The mean age of participants was 65 ± 12 years and 69% were female. The intervention increased the proportion of patients who received appropriate management within 6 months of fracture; 45% in the intervention group compared with 26% in the control group (absolute difference of 19%; adjusted OR, 2.3; 95% CI, 1.3-4.1). The proportion who had a BMD test scheduled or performed was much higher with 57% of intervention patients compared with 21% of controls (absolute difference of 36%; adjusted OR, 4.8; 95% CI, 3.0-7.0).
A centralized osteoporosis coordinator is effective in improving the quality of osteoporosis care in smaller communities that do not have on-site coordinators or direct access to osteoporosis specialists.
我们进行了一项集群随机试验,评估了一位集中协调员的效果,该协调员负责识别和跟进骨折患者及其初级保健医生的骨质疏松症情况。与对照组相比,干预组患者接受 BMD 检测的可能性增加了五倍,接受适当治疗的可能性增加了两倍。
为了确定通过电话和邮件跟进骨折患者及其初级保健医生的集中协调员(干预组)是否会增加接受适当骨折后骨质疏松症管理的患者比例,与仅接受预防跌倒的简单建议(对照组)相比。
在加拿大安大略省的小型社区医院进行了一项集群随机对照试验。每年治疗 60 至 340 名骨折患者的医院有资格参加。从急诊部记录中识别出 40 岁及以上因低创伤性骨折就诊的患者,并将其纳入试验。主要结局为“适当”管理,定义为正常骨密度(BMD)检测或服用骨质疏松症药物。
36 家医院被随机分配到干预组或对照组,130 名干预组和 137 名对照组完成了研究。参与者的平均年龄为 65 ± 12 岁,69%为女性。干预组在骨折后 6 个月内接受适当管理的患者比例增加;干预组为 45%,对照组为 26%(绝对差异为 19%;调整后的 OR,2.3;95%CI,1.3-4.1)。安排或进行 BMD 检测的患者比例也高得多,干预组中有 57%的患者,而对照组只有 21%(绝对差异为 36%;调整后的 OR,4.8;95%CI,3.0-7.0)。
在没有现场协调员或无法直接获得骨质疏松症专家的较小社区中,集中骨质疏松症协调员可有效改善骨质疏松症护理质量。