Section of Musculoskeletal Disease, Leeds Institute of Molecular Medicine, University of Leeds, Chapel Allerton Hospital, Chapeltown Road, Leeds LS7 4SA, UK.
Ann Rheum Dis. 2011 Nov;70(11):1968-74. doi: 10.1136/ard.2010.146068. Epub 2011 Jul 21.
To evaluate golimumab's effect on MRI-detected inflammation and structural damage in patients with active rheumatoid arthritis (RA) despite methotrexate (MTX).
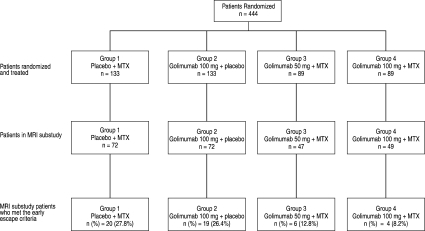
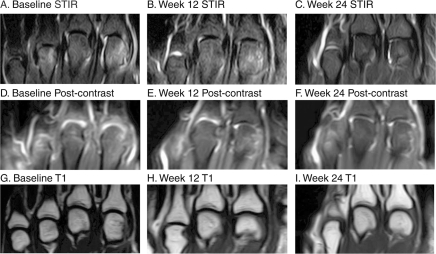
Patients (n=444) were randomly assigned to placebo plus MTX, golimumab 100 mg plus placebo, golimumab 50 mg plus MTX, or golimumab 100 mg plus MTX (subcutaneous injections every 4 weeks). A subset of 240 patients participated in an MRI substudy. MRIs (1.5T+contrast enhancement) of the dominant wrist and metacarpophalangeal (MCP) joints were obtained at baseline and weeks 12 and 24. Images were scored by two independent, blinded readers for synovitis (0-9 wrist only (n=240), 0-21 wrist+MCP (n=223)), bone oedema (osteitis) (0-69) and bone erosions (0-230) using the OMERACT Rheumatoid Arthritis MRI Scoring system.
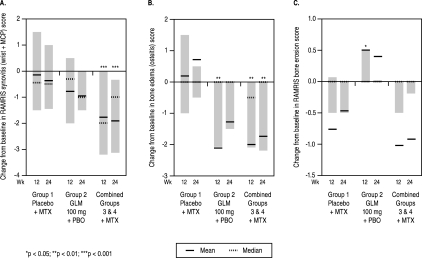
Significant improvements in synovitis and bone oedema (osteitis) were observed in the combined golimumab plus MTX groups versus placebo plus MTX at week 12 (-1.77 vs -0.15, p<0.001 wrist+MCP and -2.00 vs 0.19, p=0.003, respectively) and week 24 (-1.91 vs -0.38, p<0.001 wrist+MCP and -1.74 vs 0.71, p=0.004, respectively). Fewer than 10% of patients had a substantial degree of erosive progression (most showed no progression) across all treatment groups (including the control group), precluding adequate evaluation of golimumab's effect on bone erosions.
Golimumab plus MTX significantly improved MRI-detected synovitis and osteitis (prognosticators of future structural damage) versus placebo plus MTX at weeks 12 and 24. The effect of golimumab on bone erosions could not be determined by semi-quantitative scoring in these RA patients with minimal progression of bone erosions.
评估戈利木单抗对甲氨蝶呤(MTX)治疗失败的活动性类风湿关节炎(RA)患者的 MRI 检测到的炎症和结构损伤的疗效。
将 444 名患者随机分为安慰剂加 MTX、戈利木单抗 100mg 加安慰剂、戈利木单抗 50mg 加 MTX 和戈利木单抗 100mg 加 MTX(皮下注射,每 4 周一次)。240 名患者参与了 MRI 子研究。基线时和第 12 周和第 24 周时,对优势腕关节和掌指关节(MCP)进行 1.5T+增强 MRI 检查。由两名独立的、盲法的读者使用 OMERACT 类风湿关节炎 MRI 评分系统对滑膜炎(0-9 腕关节仅(n=240)、0-21 腕关节+MCP(n=223))、骨水肿(骨炎)(0-69)和骨侵蚀(0-230)进行评分。
在第 12 周和第 24 周时,联合使用戈利木单抗加 MTX 与安慰剂加 MTX 相比,滑膜炎和骨水肿(骨炎)均有显著改善(腕关节+MCP 分别为-1.77 对-0.15,p<0.001 和-2.00 对 0.19,p=0.003),在第 12 周和第 24 周时,滑膜炎和骨水肿(骨炎)均有显著改善(腕关节+MCP 分别为-1.77 对-0.15,p<0.001 和-2.00 对 0.19,p=0.003)。在所有治疗组(包括对照组)中,不到 10%的患者出现严重的侵蚀性进展(大多数患者没有进展),因此无法充分评估戈利木单抗对骨侵蚀的作用。
与安慰剂加 MTX 相比,戈利木单抗加 MTX 可显著改善 MRI 检测到的滑膜炎和骨炎(未来结构损伤的预测因子),在第 12 周和第 24 周时。在这些骨侵蚀进展最小的 RA 患者中,半定量评分无法确定戈利木单抗对骨侵蚀的影响。